Pathophysiology and classification of intracranial and spinal dural AVF
Article information

Abstract
Dural arteriovenous fistulas (DAVFs) are pathologic shunts between pachymeningeal arteries and dural venous channel. DAVFs are relatively rare, however, DAVFs can lead to significant morbidity and mortality due to intracranial hemorrhage and non-hemorrhagic neurologic deterioration related to leptomeningeal venous drainage. The etiology and pathophysiology of DAVFs is not fully understood. Several hypotheses for development of DAVF and classifications for predicting risk of hemorrhage and neurological deficit have been proposed to help clinical decision making according to its natural history. Herein, incidence, etiology, pathophysiology of development of intracranial and spinal DAVF including their classifications are briefly described with short historical review.
INTRACRANIAL DURAL AVF
Incidence
Dural arteriovenous fistulas (DAVFs) are pathologic shunts between pachymeningeal arteries and dural venous channel. DAVFs are distinguished from parenchymal or pial arteriovenous malformations by the presence of a dural arterial supply and the absence of a parenchymal nidus [13]. The incidence of cranial DAVFs has been estimated 0.15-0.29/100,000 per year [11] and the intracranial location is reported as transverse sinus (50%), cavernous sinus (16%), tentorium cerebelli (12%), and superior sagittal sinus (8%) [26]. DAVFs are relatively rare, accounting for 5–15% of all cranial vascular malformation. However, DAVFs can lead to significant morbidity and mortality due to intracranial hemorrhage and non-hemorrhagic neurologic deterioration related to leptomeningeal venous drainage [1,26].
Etiology
The etiology of DAVFs is not fully understood, but the majority of DAVFs in adulthood appear to be acquired. Different etiologies have been implicated such as trauma, previous craniotomy, and a hypercoagulable state including malignancy, pregnancy, infection, and prothrombotic genes [20,27,36]. DAVFs in the pediatric population are thought to be associated with congenital venous anomalies of the developing venous system or a result of birth trauma, infection, in utero venous thrombosis, or maternal hormones [30].
Pathophysiology of development of DAVFs
A meningeal branch of each artery supplying the brain or spinal cord consistently pierce the dura through a venous sinus or else are surrounded by a venous plexus. When meningeal arteries running outside the dural layers penetrate the dura, they come much closer to meningeal veins or venous sinuses running between outer periosteal and inner meningeal layer of dura.
In normal dural sinus [34], dural vessels were more numerous at angles formed by a fusion of two dural leaves, which were rich in veins of varying sizes communicating with one another. Dural arteries were not observed inside of the sinuses, but branches of veins occasionally penetrated through the sinus wall and communicated with their lumens. Even though there is no arteriovenous anastomosis among the dural vessel, the dural arteries and veins were located close to one another. This intimate relationship between the meningeal branches and the venous sinuses offers anatomical opportunity for the development of fistulas [4,39].
In histologic specimen of experimental DAVF models [34], the affected sinuses were remarkably narrowed by thickening of the intima and organized thrombi. Dural veins were markedly dilated and had communication with one another and with the lumens of the venous sinuses. No direct communication was observed between dural arteries and venous sinuses. However, fistulas were seen between arteries with a diameter of about 200 um and dilated dural veins near the venous sinuses.
While the exact mechanisms are still controversial, venous sinus thrombosis and venous hypertension have been believed to be associated with the genesis of DAVFs [5,17,36,44]. Two etiologic hypotheses regarding to sinus thrombosis and venous hypertension have been suggested. The first is that physiologic arteriovenous shunts that are normally present between meningeal arteries and dural venous sinuses expand to form a pathologic shunt in response to elevated local venous pressure as a result of sinus thrombosis [6,22]. The second is that venous hypertension due to outflow obstruction causes decreased cerebral perfusion and promotes neoangiogenesis [6,24,44]. Angiogenic growth factors, produced as a result of sinus thrombosis, might contribute to the development of DAVFs [44]. Kultulk et al. [25] proposed a three stage hypothesis for the pathogenesis of DAVFs as initial stage of venous sinus thrombosis, second stage of angiogenic factor induced microscopic fistula development within the wall of the thrombosed sinus, and final stage of recanalization of the thrombosed sinus. Whether the cause or the result of hemodynamic disturbance, venous hypertension and thrombophilic condition such as venous thrombosis clearly plays a role in the development of DAVFs [16,20]. Once triggered by venous hypertension and venous thrombosis, arterial feeder recruitment and development of DAVFs via neoangiogenesis might proceed. This process is associated with upregulation of hypoxia-inducible factor-1, vascular endothelial growth factor, stroma-cell derived factor alpha, and MMP-9 [14,16,43].
Classification
The relationship between the pattern of venous drainage and the natural history of DVAFs leads to proposal of classifications based on the venous drainage pattern of the shunts [4,7]. Borden et al. proposed a classification system incorporating spinal DAVFs on the basis of the site of venous drainage and the presence of cortical venous drainage (CVD) [4]. Spinal epidural venous plexus corresponds to an intradural sinus and the spinal perimedullary veins are subarachnoid veins. Borden type I DAVFs exhibit normal antegrade flow into the dural venous sinus or meningeal vein. Type II DAVFs are those that drain into the dural sinus with retrograde flow into the subarachnoid veins. Type III DAVFs have retrograde drainage directly into the subarachnoid veins or an isolated sinus that is completely thrombosed on both sides of the arterialized segment.
Cognard et al. have classified DAVFs into five types based on the direction of dural sinus drainage, the presence of CVD, and venous outflow architecture. Cognard Type I DAVFs have an antegrade drainage into the dural sinus without CVD. Type II DAVFs are subdivided into type IIa (retrograde drainage into a dural sinus without CVD), IIb (antegrade drainage into a dural sinus with CVD), and IIa+b (retrograde drainage into a dural sinus with CVD). Type III, IV, and V DAVFs have retrograde drainage directly into subarachnoid vein, ectatic subarachnoid vein, and spinal perimedullary vein, respectively (Table 1).

Classification of dural arteriovenous fistulas
In either classification scheme, lack or presence of CVD can allow appropriate risk prediction for therapeutic decision-making. DAVFs without CVD (Borden type I, Cognard type I, IIa) have benign natural history with mild symptoms. Annual risk of hemorrhage has been reported low [9,46]. The presence of CVD (Borden types II and III, Cognard types IIb-V) indicates an aggressive feature with an annual incidence of hemorrhage of 8% and non-hemorrhagic neurological deficit of 6-15% [21,45]. Rebleeding rate in DAVFs with CVD reaches up to 35% [10]. Subdividing DAVFs with CVD according to presence of symptoms may have more predictive value in risk stratification [46]. Asymptomatic DAVFs patients with CVD have a considerably lower annual hemorrhage risk of 1.5%, while symptomatic patients with CVD have 7.4% of annual risk. However, DAVFs has been considered to have a dynamic nature. DAVFs without CVD can develop CVD in the future with ongoing venous stenosis, thrombosis, or increased arterial flow [8,40]. Spontaneous thrombosis and resolution of DAVFs have also been reported [28].
SPINAL DURAL AVF
History and classification of spinal arteriovenous lesions
Since Foix and Alajouanine first described of spinal DAVFs (1926), the evolution of diagnostic tools has led to examine the angioarchitecture of these spinal vascular lesions better. However, there is still a lack of consensus in the classification and terminology of the spinal arteriovenous lesions [5]. Spinal vascular lesions have been described by numerous names and divided into various classifications according to clinical feature, anatomical location and angioarchitecture [41]. In general, spinal vascular lesions are divided into two categories; arteriovenous shunting lesions including spinal arteriovenous malformation (AVM) and arteriovenous fistulas (AVF), and non-shunting lesions including capillary telangiectasia and cavernous malformations. In this chapter, spinal arteriovenous shunting lesions will be further discussed.
In 1971, Di Chiro et al. described the first classification of spinal AV shunts as type I (single coiled vessel), type II (glomus), and type III (juvenile). The majority of type I fistula fit current concept of spinal DAVFs and the others correspond to intramedullary AVMs. In 1986, a direct spinal AVF (perimedullary fistula in current terminology) was added as type IV (a direct AV shunt between the anterior spinal artery and vein that was located ventral to the spinal cord). Rosenblum (1987) established most widely accepted classification: type I (dural AVF), type II (intradural intramedullary glomus AVM), type III (intradural intramedullary juvenile AVM), and type IV (intradural direct AVF) [38]. Since 1993, type IV intradural direct AVFs were described as perimedullary AVFs and perimedullary AVFs were further classified according to the number of feeding arteries and size of AVF; type I with a single feeder and single small AVF, type II with multiple feeders and multiple medium AVFs, and type III with multiple feeder and a single giant AVF [32]. Now, extradural AVFs were added in this system and subdivided into three types according to the presence of intradural venous drainage and neurological deficits [37]. Recently, Takai [42] proposed a revised version of previous classifications (Table 2). In 2008, Geibprasert and Lasjaunias reported a classification including intracranial and spinal AVFs in which AV shunts were divided into 3 groups based on the embryologic development of the venous drainage; the ventral, lateral, and dorsal epidural groups [15]. Spinal DAVFs are the lateral epidural AVFs.
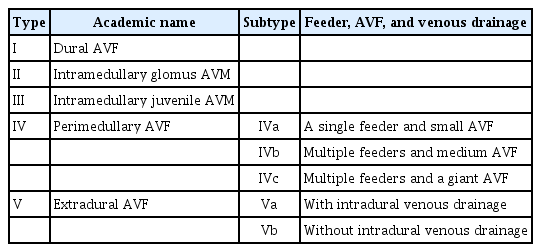
Revised classification of spinal AV shunt by Takai (2017)
Incidence and clinical characteristics
Spinal DAVFs are defined by pathologic shunt between a radicular artery and coronal venous plexus of the spine without an intervening capillary bed. They are the most common type of spinal cord vascular malformation, accounting for 50% to 85% of all spinal vascular lesions [31]. Spinal DAVFs are reported to affect 0.5-1/100,000 per year [12,23] and precise incidence of the rest of spinal vascular lesions is lacking. Spinal DAVFs are thought to be acquired lesions and preferentially affect middle-aged men. At least 80% of patients in most series are male [12]. The most frequent location is in the lower thoracic and upper lumbar area [29] and patients most commonly present with gait abnormality or lower-extremity weakness and sensory disturbances. Spinal AVM including intramedullary AVMs and perimedullary fistulas are believed to be congenital and become symptomatic in childhood or early adulthood by steal or hematoma, whereas spinal DAVF typically present in the fifth and sixth decades [38]. Perimedullary fistula is a single shunt without a nidus between the spinal artery and the spinal vein and constitutes 20% of all spinal vascular lesions. In contrast with DAVF, these lesions are located ventrally or dorsally on the spinal cord and are located intradurally but extramedullarily. Spinal subarachnoid hemorrhage is one of the occurring signs because of its intradural location, while spinal DAVF seldom presents subarachnoid hemorrhage. Intramedullary AVM presents compression effects from dilated vessels, steal phenomena, and catastrophic intramedullary hematoma in young aged patients.
Pathophysiology of development of spinal DAVFs
The pathophysiology of development of lesions and neurological deterioration is different in patients with DAVF and those with intradural spinal AVMs. Spinal DAVFs are probably acquired lesions while medullary AVM’s are congenital in nature.
Although complex pathophysiologic mechanisms underlying the development of spinal DAVFs are yet to be clarified, meningeal venous thrombosis and trauma are implicated in the development of spinal DAVFs [23]. Conditions associated with vascular fragility such as fibromuscular dysplasia [3] and neurofibromatosis type 1 [18] are associated with spinal DAVFs. Histopathological examination supported the theory of venous hypertension as a pathophysiological mechanism in the development of DAVFs and increased venous congestion as a cause of neurological deterioration [19,35].
Segmental arteries from each level of the spinal column gives rise to spinal radicular arteries supplying the dura (radiculomeningeal arteries) and accompanies the corresponding nerve root in its dural sleeve. These arteries may continue as a radiculomedullary artery, which accompanies the dorsal and ventral rami of the nerve root into the thecal sac to supply the anterior and posterior spinal arteries. An extramedullary, circumferential network of vein known as the coronal venous plexus receives spinal cord venous outflow and drains into the epidural vein via the radicular/radiculomedullary veins [5,31]. In spinal DAVFs, the radiculomeningeal artery within the dural sleeve of the nerve root fistulizes with the radicular vein and this leads to arterialize the valveless perimedullary venous plexus. An increased venous pressure, venous congestion, edema, and progressive ascending myelopathy are caused by obstruction of venous outflow [12]. An increased venous pressure results in a reduced arteriovenous pressure gradient, intramedullary impairment of autoregulation, and hypoxia [19,31]. In patients with intradural AVMs, neurological presentations are probably caused by high-pressure, high-volume, turbulent blood flow through the intradural nidus and its feeding and draining channels. Increased venous pressure as well as arterial steal attributes spinal cord ischemia due to reduction of tissue perfusion pressure [2]. Spinal epidural (extradural) AVFs are very rare, but may cause a compressive myelopathy due to a presence of a venous pouch in the epidural venous plexus. It may or may not develop venous congestion due to retrograde intradural venous drainage [33].
Notes
Disclosure
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.