


INTRODUCTION
Well-known complications of sellar tumors surgery include hypopituitarism, diabetes insipidus, hyponatremia, meningitis, cerebrospinal fluid leaks, and visual field loss. But cerebral ischemic complications after pituitary surgery are not frequently reported. They may occur after transsphenoidal or transcranial excision of the pituitary lesion via different mechanisms [3,10].
The authors present a case of a unilateral caudate infarct following pituitary adenoma resection, and through a bibliographic review based on PubMed of the cases reported in the literature to date, emphasize their presentation, etiology, and management, as well as recommendations with the aim of alerting and preventing this potential complication, rarely described in the literature, that can cause high morbidity.
CASE DESCRIPTION
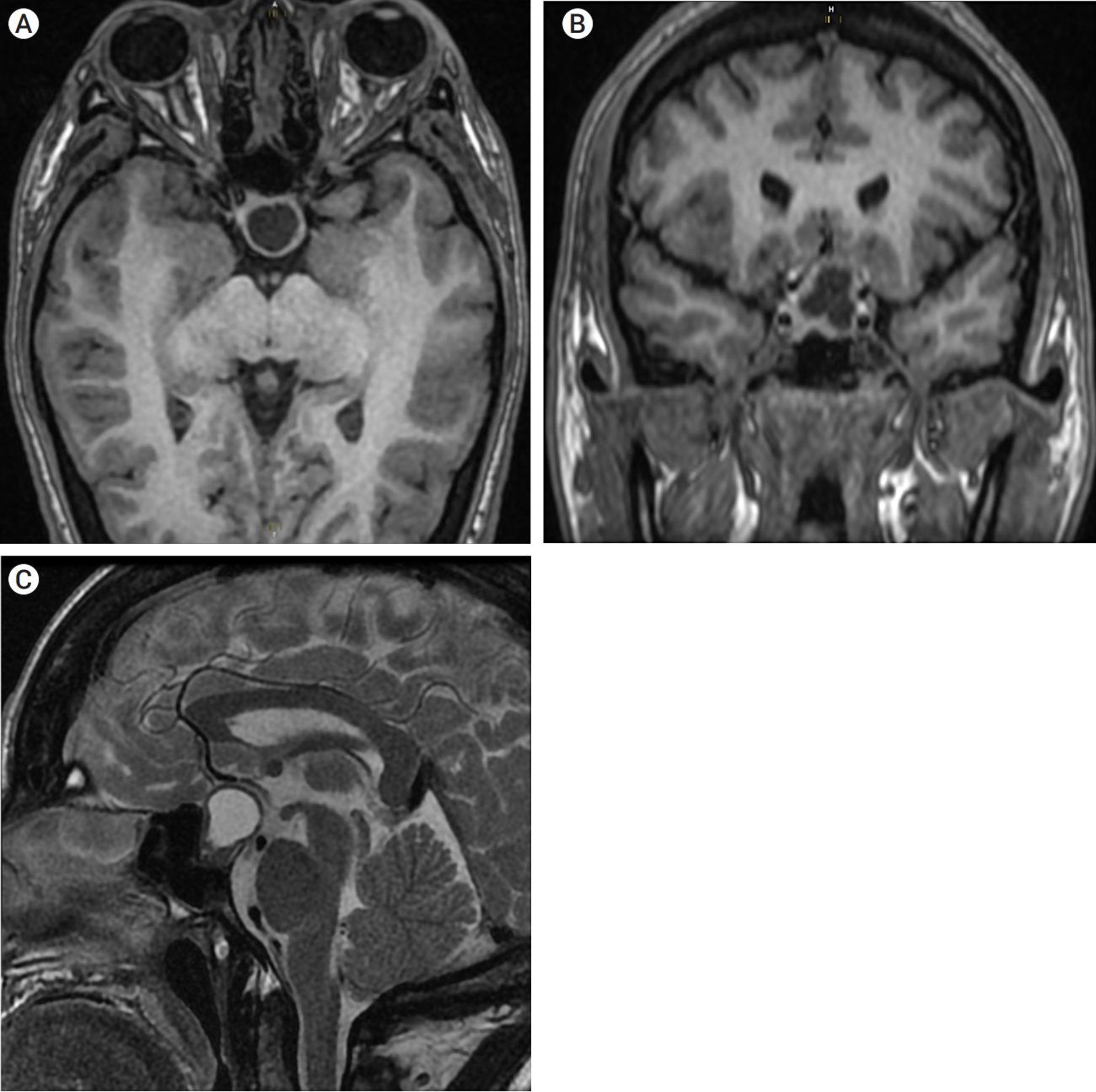
A 27-year-old female was referred to our hospital with a 5-year history of galactorrhea and menstrual disorders. A year ago, she noted that has coarse facial features and progressive enlargement of her hands and feet, as well as decreased visual acuity in both eyes. The physical examination revealed typical characteristics of acromegaly, and a bitemporal hemianopic visual field impairment. The rest of the physical examination was unremarkable. Initial laboratory tests performed showed: growth hormone (GH) 32 ng/ml (1-14); insulin-like growth factor 1 (IGF-1) 861 ng/mL (107.0-310.0); prolactin 33.9 ng/mL (3.0-18.6); thyroid-stimulating hormone (TSH) 0.27 µUI/mL (0.47-4.68); free T3 3.22 pmol/L (4.26-8.1); free T4 17.0 pmol/L (10.0-28.2); adrenocorticotropic hormone (ACTH) 20.5 pg/mL (4.7-48.8); morning cortisol 24.7 µg/dL (5 to 25); luteinizing hormone (LH) 2.15 IU/ml; follicle-stimulating hormone (FSH) 2.5 IU/ml. A magnetic resonance imaging study revealed a functional pituitary macroadenoma with suprasellar extension and compression of the optic chiasm (Fig. 1).
After completing all assessments (neuroendocrinology, neuro-ophthalmology, and neuro-otorhinolaryngology), transsphenoidal removal was performed through an endoscopic endonasal route. A total macroscopic resection was achieved, and no eventualities or lesions were reported during the intraoperative period.
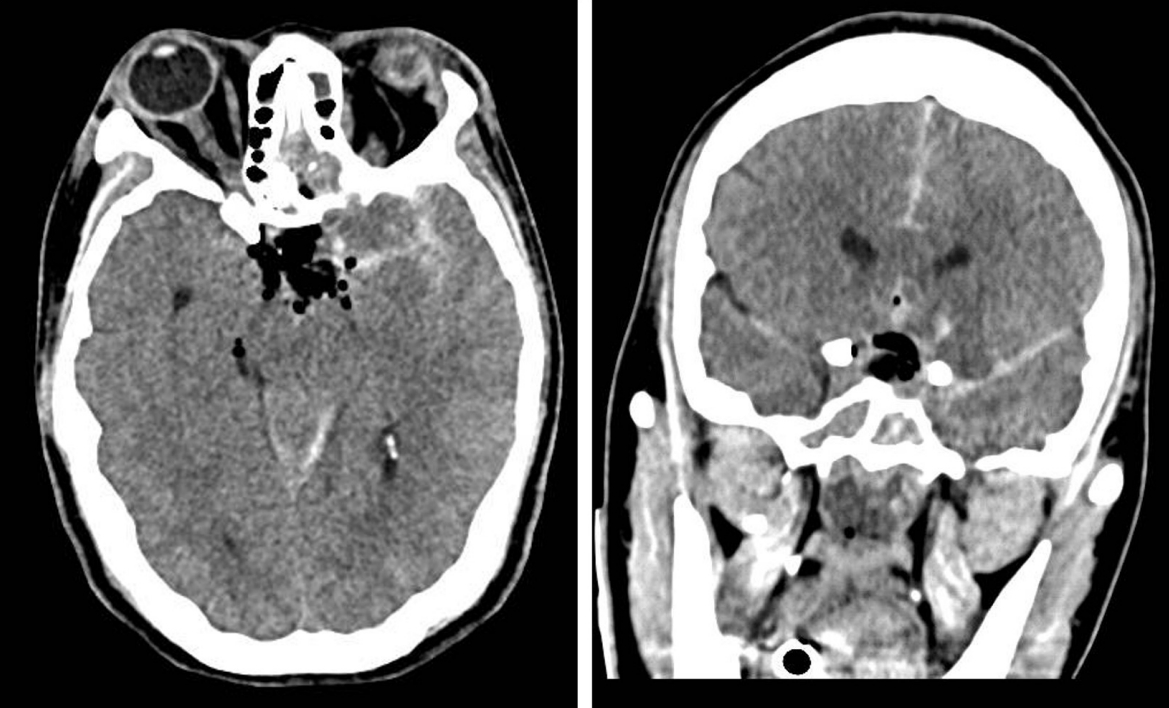
After surgery, the patient was drowsy and immediate computed tomography (CT) scan confirmed total tumor removal, with associated postoperative changes in addition to a subarachnoid hemorrhage (SAH) modified-Fisher 3 (Fig. 2).
The usual perioperative hydrocortisone stress dose was administered before and after surgery, and her fluid status, serum sodium, serum and urine osmolality were monitored every 8 hours. During the first postoperative (PO) day, the patient presented events of diabetes insipidus requiring a dose of desmopressin and was controlled on the third PO day. By day five, the patient continued to be unusually drowsy, and the physical examination revealed altered mental status (Glasgow coma scale: 13), dysarthria, and paresis of the right arm (Medical Research Council grade 3). A cranial CT was performed revealing hypoattenuation in the head of the left caudate nucleus (Fig. 3). Being a young woman with no medical history, and the subarachnoid hemorrhage being the most specific finding, the medical team suspected that it could be an event of ischemia associated with vasospasm. Complementary management was established including fluid optimization, blood pressure control and nimodipine 40 mg every 6 hours. Until this day, the patient was maintained on medication that included an anticoagulant and prednisone 5 mg/day, and no further episode of diabetes insipidus occurred, for which desmopressin had been discontinued. By day 10, her mental status improved but she maintained drowsiness and motor weakness. She was discharged on day 11 conscious but dependent for routine activities (modified Rankin 3).
DISCUSSION
Proximity of a pituitary tumor to circle of Willis and distal segments of the internal carotid artery (ICA) makes the surgical excision vulnerable to vascular complications, such as SAH, vasospasm, and ischemic strokes. However, ischemic complications are relatively infrequent [10]. They may occur after transsphenoidal or transcranial excision of the pituitary lesion via different mechanisms: (1) direct trauma to the vessel wall, (2) mechanical compression of the vessels, (3) vasospasm secondary to SAH or tumor secretion of vasoactive agents, or (4) hypothalamic injury [4,10]. Some characteristics of the tumor such as size, supra or retrosellar extension, as well as the presence of pituitary apoplexy, have also been associated with vascular postoperative complications [7].
In the reported case, the patient presented a selective infarction of the head of the left caudate nucleus, which topographically corresponds to the territory irrigated by the recurrent artery of Heubner (the largest perforating branch from the proximal anterior cerebral artery [ACA]; its origin is near the A1-ACom-A2 junction of the ACA, arising from the proximal A2 in 90% of cases, and from the distal A1 in 10% of cases) [6]. Caudate nucleus is important in the modulation of motor actions and influences associative and cognitive processes. Its functional anatomy has been well described in the literature [2,11,12].
So, what could have caused this complication? We consider that direct trauma or mechanical compression was not the cause in this patient since this vessel is anatomically located more dorsal and lateral than the extension of the actual tumor that didn’t have overwhelming dimensions. Another cause that we could rule out is the interaction of vasoactive chemicals released from the tumor or the hypothalamo-hypophyseal area, hypothalamic manipulation or damage, which has been associated as a vasospasm-inducing mechanism, even in the absence of SAH. However, these are hypotheses that are still unclear, and are more frequently described in macroadenomas and pituitary apoplexy [14].
Analyzing the literature and reported cases, as well as the experience of the surgeons at our institution, the authors consider that vasospasm is the mechanism that could best explain what was presented in the reported case, since post-surgical blood in the resection cavity extends through the subarachnoid cisterns and could cause this spastic response in the cerebral vessels.
We found that one of the first descriptions of cerebral vasospasm following pituitary surgery was described in 1980 by Camp et al.; suggesting that subarachnoid hemorrhage with direct extension into the basal cisterns or the fat/synthetic material influence on the basal cisterns could be a cause of cerebral vasoespasm [4]. Puri et al. also stated that patients with large macroadenomas with significant suprasellar extension who underwent a subtotal resection with postoperative blood within the tumor capsule and subarachnoid space were more susceptible to vasospasm [13]. In a study conducted by Estakhr et al., vasospasm occurred more frequently in anterior than in the posterior circulation; compared to the other arteries, anterior cerebral artery was the most involved artery (72%), and multiple territories vasospasm (ACA and medial cerebral artery and ICA) was reported in 36% of all cases; the data showed that unilateral vasospasm was detected more frequently than bilateral spasm (64% vs 36%) [9].
Despite findings reported, we found that the risk for vasospasm/delayed cerebral ischemia (VS/DCI) following macroadenoma surgery is likely multifactorial, where tumor size, location, vessel involvement, and evidence of postoperative bleeding may all contribute. A literature review found that VS/DCI can occur in both transcranial and transsphenoidal approaches and the most common risk factors are vessel involvement, post-operative subarachnoid bleeding, and tumor suprasellar extension [1,8,13]. The radiographic findings of VS/DCI after pituitary surgery has been reported to range from 3 days to 2 weeks after surgery.8 In our report symptom onset began on PO day 5.
Multiple guidelines have established the optimized management of VS/DCI in aneurysmal SAH, but none in cases associated with postoperative pituitary surgery. Hemodynamic augmentation therapy using hypertension and euvolemia, thromboxane A2 antagonists, calcium channel blockers, endovascular angioplasty, or intra-arterial vasodilators, and intrathecal thrombolytics, has been well described in the literature [5,8-10]. Unfortunately in this patient, the condition was suspected when a cerebral infarction had been established, however management was initiated to prevent a new episode. This leaves us with the message that in patients who experience or persist with neurological deterioration, vascular etiology should be considered as a potential cause of their condition, so that it can be identified and treated early.
The uniqueness of this case is the unusualness, reflected in the few cases previously reported. Postoperative focal infarcts have more commonly been described as occurring due to direct vascular injury, which does not appear to be the cause in this case because this was not evident during surgery. One of the objectives of this report is the educational value it can leave regarding vascular complications that may occur in this type of surgery; a limitation was not having studies such as angioCT or Doppler ultrasound that document the aforementioned, however, due to the history and clinical evolution, it should guide us to think of vasospasm as a potential etiology due to the documented subarachnoid bleeding, presenting within the time range usually described in the literature.
The authors can recommend the following key lessons: 1) SAH can be produced in “aggressive” procedures where the arachnoid is opened, especially those such as functional adenomas where total resection is required; 2) Applying effective hemostasis and ample irrigation during the procedure may minimize the amount of subarachnoid blood leaking into the basal cisterns which may reduce the occurrence of vasospasm; 3) Postoperative SAH should be monitored in specialized units since it can carry risk of vasospasm as occurs with aneurysmal SAH, and if incipient signs of DCI are present, it should be treated according to the guidelines regardless of the etiology. A good outcome can be achieved if detected early and managed judiciously with fluid management and supportive care.
CONCLUSIONS
Vasospasm and delayed cerebral ischemia following pituitary surgery can occur either via transcranial or trans nasal endoscopic route and can generate devastating complications associated with ischemic events, increasing neurological morbidity, and prolonging the hospital stay significantly. Key warning signs postoperatively could indicate increased risk for cerebral vasospasm and must be recognized in a timely manner, with appropriate treatment strategies implemented once these symptoms present.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






