



INTRODUCTION
Multiple intracranial aneurysms, corresponding to 15-25% of cerebral aneurysms, are relatively frequent among the vascular diseases of the central nervous system [3]. Posterior communicating (pComm) aneurysms represent 15 to 25% of intracranial aneurysms [10]. Bilateral pComm aneurysms (“mirror aneurysms”) are rare, representing only 2% of the mirror intracranial aneurysms, thus being a true neurosurgical challenge [1], with only a few cases reported in the current literature [7]. In this article, we present a patient with mirror pComm aneurysms in which both lesions were treated through a single approach, followed by a brief review of the literature.
CASE REPORT
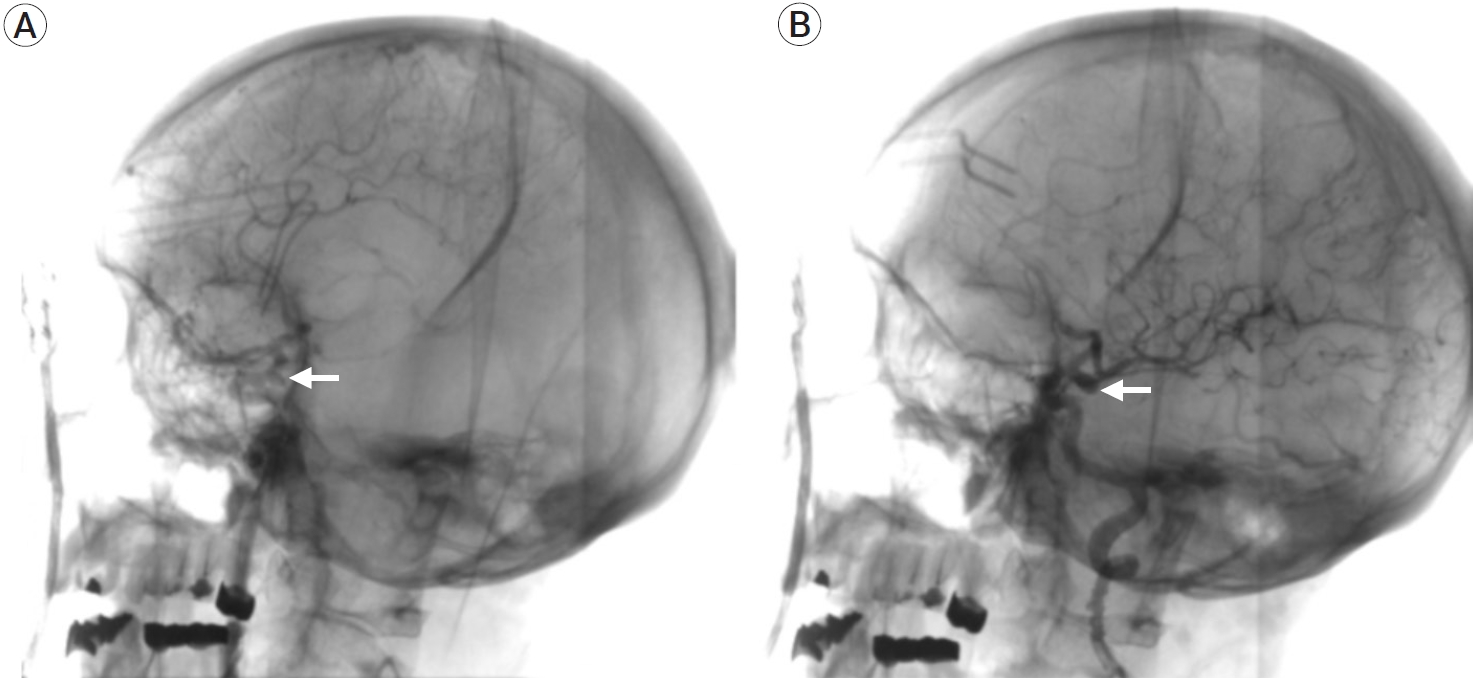
A 50-year-old female patient with no previous medical background was admitted to our institution after presenting recurrent episodes of non-specific headache and horizontal diplopia. Neurological examination revealed a Glasgow Coma Scale (GCS) of 15 (M6, V5, O4), and a left oculomotor palsy, with no further disturbances. Non-contrast computed tomography (CT) and an angioCT scans revealed bilateral aneurysmatic lesions in both internal carotid arteries (ICA) communicating segments. A digital subtraction angiography (DSA) was performed in order to get a better anatomical definition of both aneurysms (Fig. 1). We decided to perform a left pterional approach in order to gain access to the symptomatic lesion at first instance, and if anatomical findings were optimal, a contralateral clipping would be sought for the right aneurysm. It is essential to mention that this procedure was performed in a hybrid operating room (HOR) with DSA before clipping, roadmapping assistance during both dissection and clipping, and an immediate postclipping DSA to assess distal vascular permeability and vasospasm.
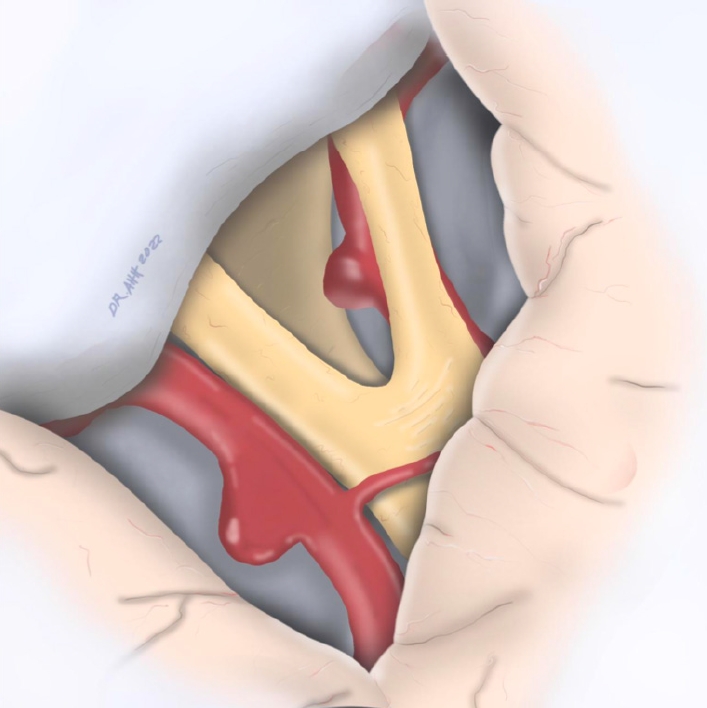
During subarachnoid dissection, a post-fixed optic chiasm with a wide interoptic space was identified (Fig. 2), which allowed a complete dissection of the arachnoid planes, with complete visualization of the contralateral aneurysm’s neck and collateral arteries of the contralateral ICA (pComm and anterior choroidal artery) (Fig. 3). After thorough, the ipsilateral aneurysm was clipped with no difficulty, assessing patency of the ICA branches (Fig. 4) with DSA (Fig. 5). Both aneurysms were permanently clipped with a 7 mm straight clip. The patient’s postoperative course was uneventful, with a sequel left oculomotor palsy.
DISCUSSION
Multiple intracranial aneurysms represent around 15-30% of all aneurysms [9]. Mirror aneurysms represent about 2 to 12% of the latter, being the pComm location the third most frequent [6]. Previous studies have described the site of the lesion and the clinical characteristics of mirror aneurysms, however, results differ. Meissner et al. [6] found that mirror aneurysms are more extensive than single aneurysms. In contrast, Lee et al. [4] found that mirror aneurysms are smaller than their counterparts.
Risk factors associated with mirror aneurysms are female sex, smoking, alcohol consumption, and genetic variables that directly influence their growth because of the hemodynamic stress in the aneurysm wall [2,5,10].
Although studies have fully analyzed the clinical characteristics, risk factors, and incidence of mirror aneurysms, there is not a consensus about the appropriate approach to these lesions. Many authors have proposed various approaches for bilateral pComm aneurysms. Some include endovascular therapy for both lesions, endovascular therapy for the non-ruptured lesion and clipping for the ruptured one, or clipping by bilateral approaches [8]. These approaches are selected whereas there is a ruptured aneurysm, its location, the size of its neck, and the patient’s neurological condition. However, the criteria for treatment need to be better defined as there is still controversy about the appropriate management.
Unilateral approaches for bilateral pComm aneurysms have been described only in case reports [7]. However, most neurosurgeons prefer unilateral approaches for unilateral lesions without rupture because of the manipulation and mobilization of the surrounding structures. Likewise, the single approach is technically complex because the angle of view of the contralateral neck can be slight. In addition, cerebral edema can make managing the surgical space more challenging in ruptured aneurysms.
In our case, we can observe how the unilateral approach can be implemented in selected cases of bilateral pComm aneurysms because the wide interoptic space allows us to visualize the neck of the contralateral aneurysm achieving a correct clipping. Some anatomical factors that allow complete visualization of the contralateral neck are a wide interoptic space and a post-fixed chiasm. However, it should be mentioned that only during surgery can we judge whether these anatomical factors and cerebral edema can provide enough space to maneuver on the contralateral side and perform the clipping. Future studies should be performed using preoperative magnetic resonance image measurements to determine whether we can use the unilateral approach routinely.
We consider this technique is less expensive than bilateral endovascular approaches and less morbid than bilateral craniotomies because the surgical time is reduced and a single incision is made. Likewise, it is unnecessary to expose the patient to two surgical times for combined approaches (endovascular and clipping at different times).
CONCLUSIONS
Unilateral approaches for bilateral pComm aneurysms can be feasible, safe, and less expensive than other approaches. However, it is imperative to remember that visualization of the contralateral neck of the aneurysm, grade of cerebral edema, and experience of the neurosurgeon are factors that carry out a good clipping. In addition, it is necessary to have full vascular anatomical knowledge and the use of the technological tools available to perform effective and safe surgery.



 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






