Alterations of vital signs as prognostic factors after intraprocedural rupture of intracranial aneurysms during endovascular treatment
Article information

Abstract
Objective
To report our experience with intraprocedural rupture (IPR) of intracranial aneurysms during endovascular treatment and evaluate alterations in vital signs as independent prognostic factors to predict the outcomes of IPR.
Methods
Between January 2008 and August 2021, 34 patients (8 ruptured and 26 unruptured) were confirmed to have IPR based on our dataset with 3178 endovascular coiling procedures. The patients who underwent additional surgeries related to IPR were classified as the OP group (n=9), while those who did not receive additional surgeries were classified as the non-OP group (n=25). Vital signs were recorded during the procedure by anesthesiologists and analyzed.
Results
Of the 34 patients included in this study, eight initially presented with subarachnoid hemorrhage due to a ruptured aneurysm. The clinical outcomes at discharge were significantly different between the two groups (p=0.046). In the OP group, five patients showed favorable outcomes at discharge, while four showed unfavorable outcomes. In the non-OP group, 23 patients showed favorable outcomes at discharge while two patients showed unfavorable outcomes. Maximal (MAX) systolic blood pressure (SBP) (odds ratio [OR] 1.520, 95% confidence interval [CI] 1.084-2.110; p=0.037) and higher differential value MAX-median blood pressure (MBP) (OR 1.322, 95% CI 1.029-1.607; p=0.044) remained independent risk factors for poor prognosis after IPR on multivariate logistic regression analysis.
Conclusions
The MAX SBP and the difference between the maximal and baseline values of MBP are key factors in predicting the prognosis of patients after IPR, as well as providing useful information for predicting the outcome. Further research is required to confirm the relationship between naive pressure and prognosis.
INTRODUCTION
Endovascular treatment such as coil embolization has become a main treatment option for unruptured or ruptured cerebral aneurysms. The incidence of intraprocedural rupture (IPR) tends to increase as endovascular treatment is widely accepted in multiple institutions to treat aneurysms [10,12]. Based on previous studies, the incidence of IPR for ruptured aneurysms was between 0% and 16.1%, while that for unruptured cases was between 0% and 4% [12]. It is also considered to be the most severe complication with mortality rates reported to be up to 33% based on a meta-analysis [5,6]. Endovascular treatment is a procedure performed without opening the patient’s skull. IPR is a condition characterized by aneurysmal rupture. This situation can increase intracranial pressure and cause acute hydrocephalus afterward [13]. In addition, it can cause an alteration of vital signs during endovascular procedures. This study aimed to report our experience with IPR and evaluate alterations in vital signs as independent prognostic factors to predict the outcomes of IPR.
MATERIALS AND METHODS
Patient selection
This retrospective study was approved by our Institutional Review Board, and informed consent was waived. Between January 2008 and August 2021, we prospectively constructed a database containing a series of 3178 aneurysms (486 ruptured and 2692 unruptured) managed with endovascular treatment. Among them, 34 cases (8 ruptured and 26 unruptured) were confirmed to have ruptured during the procedure and were included in this study. All patients met the following criteria: (1) underwent endovascular treatment for intracranial aneurysms and (2) had confirmed IPR. The exclusion criteria were as follows: presence of a (1) traumatic pseudoaneurysm, (2) blood blister-like aneurysm, and (3) dissecting aneurysm.
Based on radiological records, IPR was defined as contrast extravasation during the procedure. Poor prognosis after IPR was defined as the need for additional surgeries, such as external ventricular drainage (EVD) or decompressive craniectomy related to IPR. According to the definition, the OP group (n=9) comprised patients who received additional surgeries related to IPR, and the non-OP group (n=25) comprised those who did not undergo additional surgeries. We reviewed the vital signs during the procedure, while a patient was under general anesthesia. Additionally, patient and aneurysm characteristics, such as sex, age, location and size of the aneurysm, hypertension, diabetes, dyslipidemia, smoking, and alcohol consumption were retrospectively reviewed and analyzed to evaluate risk factors for predicting the prognosis of IPR. Clinical outcomes were assessed using the modified Rankin Scale (mRS) on the time of discharge. A favorable outcome was defined as a mRS score of 0-2, and an unfavorable outcome was defined as a mRS score of 3-6. A mRS score of 6 indicated death.
Vital signs during general anesthesia
Systolic blood pressure (SBP), median blood pressure (MBP), diastolic blood pressure (DBP), heart rate (HR), and pulse pressure (PP) were recorded by anesthesiologists during the procedure. The maximal and minimal values of SBP, DBP, MBP, HR, and PP were selected for each patient, and the differences between the values and the baseline values were calculated. Because some of the differences were in terms of negative values, the root mean square (rms) was measured to determine the average of the differences. Baseline vital signs (baseline SBP, MBP, DBP, HR, and PP), maximal vital signs (MAX SBP, MAX DBP, MAX MBP, MAX HR and MAX PP), minimal vital signs (MIN SBP, MIN DBP, MIN MBP, MIN HR and MIN PP), differential values between the maximal or minimal vital signs and baseline values (dMAX-SBP, dMAX-MBP, dMAX-DBP, dMAX-HR, dMIN-SBP, dMIN-DBP, dMIN MBP, and dMIN HR), and root mean square values (rms dSBP, rms dDBP, rms dMBP, and rms dHR) were recorded and analyzed.
Endovascular treatment
All endovascular procedures were performed under general anesthesia. A 6-Fr or 7-Fr guiding catheter was positioned in the internal carotid artery via the common femoral artery for anterior circulation aneurysms or in the vertebral artery for posterior circulation aneurysms. While treating ruptured intracranial aneurysms, heparin was not injected intravenously or subcutaneously but was mixed into the saline flushes during the procedure. When stent-assisted coiling would be expected, loading doses of clopidogrel (300-600 mg) and aspirin (200-400 mg) were given via a nasogastric tube immediately after femoral artery puncture. For elective procedures involving unruptured aneurysms, heparin (50 U/kg) was injected intravenously immediately after the femoral puncture. Patients were taking a daily dosage of 75-mg clopidogrel and 100-mg aspirin for more than 5 days before the procedure. When simple coiling was performed without stents, the patients were not prescribed antiplatelet agents after the procedure. When stent-assisted coiling was performed, patients were prescribed 75 mg of clopidogrel daily for 3-9 months and 100 mg of aspirin daily for a minimum of 12 months after the procedure.
Statistical analysis
The IBM SPSS (version 25, SPSS Inc., Chicago, IL, USA) was used for the statistical analysis. The values were expressed in terms of average standard deviation. Chi-square analysis was performed to determine significant differences based on categorical variables. The continuous variables did not follow a normal distribution. The Mann-Whitney U test was performed to determine statistical significance. The p-value, exponentiation of the B coefficient, and 95% confidence intervals were calculated using multivariable logistic regression. Multivariate logistic regression was performed to determine the risk factors that could be used to predict prognosis after IPR.
RESULTS
Of the 34 patients included in this study, the mean age was 58.8±10.3 years and 27 patients were female. Eight patients initially presented with subarachnoid hemorrhage (SAH) due to a ruptured aneurysm and they all had a good Hunt and Hess grade (Hunt and Hess grade 2 in five patients and grade 3 in three). No patient underwent EVD prior to endovascular treatment of the aneurysm.
Table 1 presents detailed characteristics of the two groups. There was no significant difference between the two groups in categorical values, such as sex, age, location of the aneurysm, aneurysmal size, hypertension, diabetes mellitus, dyslipidemia, smoking, and alcohol consumption history. However, the clinical outcome at discharge was significantly different between the two groups (p=0.046). In the OP group, nine patients underwent additional surgeries to control intracranial pressure; six patients underwent EVD and three underwent decompressive craniectomy. Among them, five patients showed favorable outcomes (mRS 0-2) at discharge while four patients showed unfavorable outcomes: mRS score 3 in one, mRS score 4 in two, and mRS score 6 (death) in one. In the non-OP group, 23 patients showed favorable outcomes at discharge while two showed unfavorable outcomes: mRS score 3 in one and mRS score 6 in one.

Characteristics of patients who experienced intraprocedural rupture
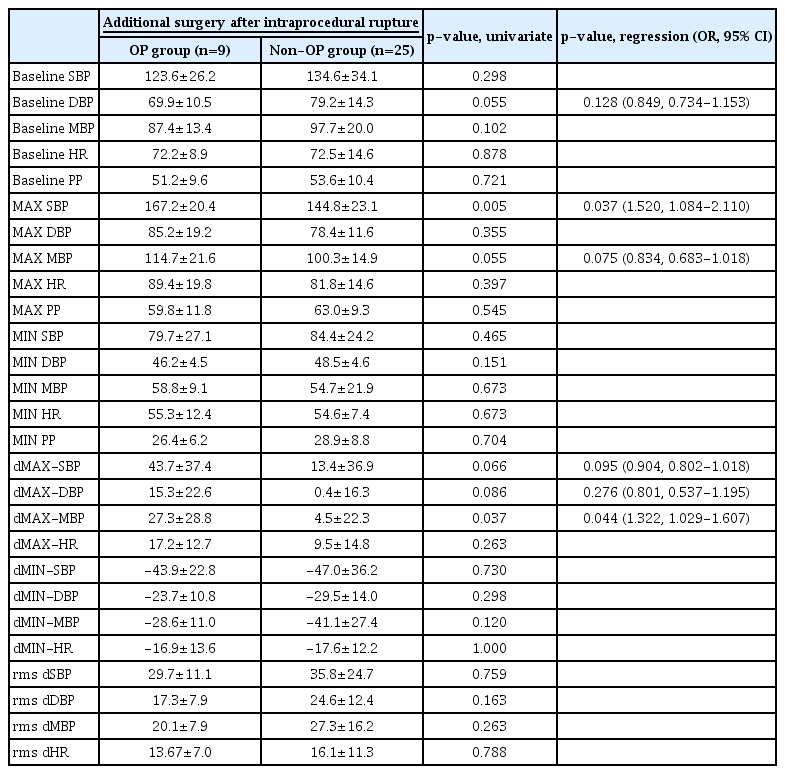
The baseline vital sign values did not show significant differences between the two groups (SBP, DBP, MBP, HR, and PP: p=0.298, 0.055, 0.102, 0.878, and 0.721 respectively; Table 2). MAX SBP and dMAX-MBP were the key values that showed statistical significance. The OP group tended to reveal higher MAX SBP (167.2±20.4 mmHg) and higher dMAX-MBP (27.3±28.8 mmHg) compared to those of the non-OP group (144.8±23.1 mmHg, p=0.005, and 4.5±23.3 mmHg, p=0.037, respectively). Baseline DBP, MAX SBP, MAX MBP, dMAX-SBP, dMAX-DBP, and dMAX-MBP, with a p-value of <0.10 in the univariate analysis (p=0.055, 0.005, 0.055, 0.066, 0.086, and 0.037, respectively), were included in the multivariate logistic regression analysis to determine independent associations of poor prognosis after IPR with other factors. MAX SBP (odds ratio [OR] 1.520, 95% confidence interval [CI] 1.084-2.110; p=0.037) and higher dMAX-MBP (OR 1.322, 95% CI 1.029-1.607; p=0.044) remained independent risk factors for poor prognosis after IPR in the multivariate logistic regression analysis (Table 2).
Risk factors for the poor prognosis after intraprocedural rupture
DISCUSSION
In the present study, IPR occurred in approximately 1.1% (34/3178) during endovascular treatment of intracranial aneurysms: 1.6% (8/486) in ruptured aneurysms and 1.0% (26/2692) in unruptured aneurysms. The OP group with additional operations after IPR tended to have higher SBP and dMAX-MBP values during the procedure. SBP showed great potential as an independent factor for predicting IPR prognosis. To the best of our knowledge, this is the first study to evaluate the prognostic factors for IPR. We speculated that a poor prognosis could be expected if the patient showed high MAX SBP and dMAX-MBP.
There are several reports on the risk factors for IPR. Kwon et al. reported the relevance of aneurysm location to IPR. The anterior communicating artery showed a higher incidence of IPR than other locations, which can be explained by the difficulty of accessing the point of the aneurysm [9]. In addition, aneurysmal size was another important factor affecting IPR. Smaller-sized aneurysms showed a higher rate of rupture during the procedure [9,12]. The mechanism of IPR is related to several factors such as herniation of the coil mass and increased pressure of the artery due to contrast injection during the procedure [5]. It is a critical complication of endovascular treatment, and even experienced intuitions are always exposed to the risk of IPR [4]. However, no study has considered predicting the prognosis of IPR, especially considering vital signs during the procedure.
SAH occurs due to a ruptured aneurysm in the space under the cranium. It is impossible to expand the intracranial volume because of the hard bony structure of the cranium. After rupture of an aneurysm, if the volume of SAH is sufficient to occupy a certain volume of the intracranial space, the intracranial pressure would increase. The Cushing reflex is a well-known symptomatic phenomenon in patients with increased intracranial pressure. Bradycardia, increased pulse pressure, and irregular respiration are the triad symptoms of the Cushing reflex. Patients with SAH and Cushing reflex are known to have almost two-fold higher mortality than those without the Cushing reflex [1].
SAH and IPR share common pathological situations and processes. The only difference is that IPR occurs during interventions. Therefore, this study focused on vital signs, especially the widened pulse pressure and respiration rates related to the Cushing reflex, which were recorded by anesthesiologists during the procedure.
We assumed that increased pulse pressure is related to poor outcomes after IPR. However, the difference between the pulse pressures was not the key value, but the maximal naive pressure was. Unexpectedly, the MAX SBP and the difference between the maximal and baseline values of MBP were significantly different between the two groups. Based on multivariable logistic regression analysis, the MAX SPB value was the most critical factor. A higher naive blood pressure after the first rupture of an aneurysm during the procedure injures the central nervous system more fatally. This indicates that naive pressure plays a key role in influencing the brain parenchyma. Arima et al. prospectively reported the importance of controlling blood pressure in cases of hemorrhagic stroke. The well-controlled blood pressure group showed a smaller infarct area, which led to a better prognosis [8]. This might be a clue to the relationship between blood pressure and brain parenchymal damage. After a rupture, the Cushing reflex may start as a response to the central nervous system injury. This was probably another reason why patients with higher SBP had more fatal outcomes.
No study has dealt with the risk factors for poor prognosis after IPR based on vital signs. Previous studies have focused on the risk factors for or mechanisms of IPR. However, there are several reports considering the importance of blood pressure in the case of trauma [2,3,7,11]. In patients with brain trauma, a higher blood pressure is statistically associated with poor prognosis. The authors hypothesized that it was related to the Cushing reflex [2]. Ley et al. reported that elevated SBP after blunt trauma was a predictive factor for mortality. An elevated blood pressure was related to a delayed discharge rate and pneumonia [11]. Based on a previous study, monitoring vital signs during the interventional process could be a good indicator to study the prognosis of IPR. Elevated SBP is indicative of a poor prognosis after IPR.
The limitations of this study include its retrospective nature and small sample size. The data were from two different neurovascular institutions. This may have caused selection bias during the analysis. Additionally, the small sample size reduced the representativeness of the sample. Finally, obliteration time from IPR to complete obliteration of the aneurysm and other procedure related factors, such as types of guide wires, types of coils, types of microcatheters, or types of stents, were not evaluated, which would affect outcomes.
CONCLUSIONS
The MAX SBP and the difference between the maximal and baseline values of MBP were the key factors in predicting the prognosis of patients after IPR and provide useful information for predicting the outcomes. To the best of our knowledge, this is the first report to emphasize the importance of naive pressure during IPR. Further research is required to confirm the relationship between naive pressure and prognosis.
Notes
Disclosure
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.