Diffusion-weighted imaging-positive lesions following endovascular treatment for ruptured and unruptured aneurysms: Its incidence according to antithrombotic drugs
Article information

Abstract
Objective
Microembolic infarcts are frequently observed on diffusion-weighted imaging (DWI) following endovascular treatment. We investigated DWI-positive lesions and symptomatic ischemic complications (SICs) in patients with ruptured and unruptured aneurysms following coiling and the relationship between DWI-positive lesions and antithrombotic drugs.
Methods
Between January 2016 and December 2020, 83 patients underwent DWI within 48 h following endovascular treatment for ruptured (n=30) and unruptured (n=53) aneurysms.
Results
The overall rate of DWI-positive lesions was 55.4%. There were no significant differences in the occurrence rate (45.3% vs. 43.3%, p=1.000) and the number of lesions (2.7±4.6 vs. 4.0±5.3, p=0.237) between unruptured and ruptured aneurysms. SIC occurred more frequently in patients with ruptured aneurysms than unruptured ones (20.0% vs. 1.9%, p=0.015). The cutoff value of DWI-positive lesions for predicting SIC was 5 (sensitivity 100%, specificity 78.9%). The procedure time was significantly longer in patients with DWI-positive lesions ≥5 than those with DWI-positive lesions <5 (104.1±43.8 vs. 85.1±30.8 min, p=0.030). Patients with DWI-positive lesions <5 were more frequently observed in the postprocedural heparinization group than in the no heparinization group (85.7% vs. 58.5%, p=0.012).
Conclusions
The incidence of DWI-positive lesions did not differ significantly between the ruptured and unruptured aneurysms. However, SIC occurred more frequently in patients with ruptured aneurysms. Longer procedure time is a risk factor for DWI-positive lesions, and postprocedural heparinization seems to reduce the incidence of DWI-positive lesions.
INTRODUCTION
Microembolic infarcts appearing as tiny high-signal intensity lesions on diffusion-weighted imaging (DWI) are often observed after endovascular procedures. Previous studies have reported that the rate of ischemic lesions on DWI ranges from 10% to 77% following endovascular treatment for intracranial aneurysms [1,5,7,10,15]. Most patients with microembolic infarcts are asymptomatic, and the clinical significance of these lesions remains controversial. However, these microembolic infarcts reflect damage to brain tissue.
Antiplatelet preparation and heparinization are critical for preventing thromboembolic complications [17,18]. Antiplatelet preparation is accepted as standard therapy in coil embolization for an unruptured aneurysm [6,24]. Several studies have shown that heparin infusion during or after the procedure is safe and effective in patients with ruptured aneurysms [3,8,26]. However, there has been little research on the incidence of microembolic infarcts according to antithrombotic agents.
We investigated the incidence of DWI-positive lesions in patients with ruptured and unruptured aneurysms following endovascular treatment. In addition, this study evaluated the relationship between DWI-positive lesions and symptomatic ischemic complications (SIC) and the incidence of DWI-positive lesions according to antithrombotic drugs.
MATERIALS AND METHODS
Patient population and characteristics
The Institutional Review Board approved this retrospective study (SCMC 2021-01-002) and waived the requirement for informed consent. We contacted 304 patients treated with endovascular procedures for intracranial aneurysms between January 2016 and December 2020. Patients who underwent DWI within 48 h after the procedure were included in the study. Parent artery occlusion, hypoxic brain damage due to increased intracranial pressure, and branch artery occlusion due to coil protrusion were excluded. Ninety-seven patients underwent DWI within 48 hours. Among them, six patients were excluded due to parent artery occlusion, four due to hypoxic brain damage, and four due to branch artery occlusion. Finally, 83 consecutive patients were included in the study.
We evaluated multiple baseline factors previously associated with patient outcomes after the procedure. Outcome measures included developing high-signal intensity on DWI, SIC, 3-month modified Rankin Scale (mRS) score, complications after additional surgery, and heparin-induced thrombocytopenia (HIT). SIC was defined as any new neurological decline, such as hemiparesis, facial palsy, aphasia, and dysarthria, consistent with a DWI-positive lesion within 1 week after the procedure.
Endovascular treatment and antithrombotic drugs
All procedures were performed under general anesthesia. For unruptured patients, dual antiplatelet medication (aspirin, 100 mg, and clopidogrel, 75 mg) was started 5–7 days before the procedure. If antiplatelet therapy was not administered, a loading dose of aspirin and clopidogrel (aspirin, 300 mg, and clopidogrel, 300 mg) was administered the day before the procedure. At the beginning of the procedure, a heparin bolus (3000–5000 IU) was administered intravenously, depending on the patient’s weight. The activated coagulation time was maintained between 2 and 3 times during the procedure.
Patients with aneurysmal subarachnoid hemorrhage (SAH) underwent endovascular treatment as soon as possible, predominantly within 1 day after admission. Dual antiplatelet preparations were not administered to patients with a ruptured aneurysm. An intravenous bolus of heparin was administered after the dome was secured. Extra ventricular drainage (EVD) or lumbar drainage was performed and maintained for 7–14 days after the procedure.
Patients were assigned to one of three attending cerebrovascular neurosurgeons, only one of whom favored postprocedural heparinization. For patients undergoing postprocedural heparinization, an infusion of unfractionated heparin was started immediately after the procedure. The activated partial prothrombin time was monitored every 4 h and targeted between 50s and 70s for 24 h.
MRI protocol and outcome evaluation
Within 48 hours after the procedure, DWI was performed to check for any silent thromboembolic events, regardless of any neurological changes. In patients who underwent continuous heparinization, DWI was performed within 24 h after discontinuation. If hyperacute ischemic lesions on DWI were observed, the apparent diffusion coefficient values in the corresponding region were correlated with the findings. We then identified the lesion size, number, and location, including both target and non-target areas. Although there were no size criteria for the DWI-positive lesions, we regarded a lesion larger than 10 mm in maximum diameter as an obvious infarct. All DWI-positive lesions, including obvious infarct lesions, were counted by the reader.
Angiographic occlusion assessment was classified using the simplified Raymond classification scale (1: complete obliteration, 2: residual neck, 3: residual aneurysm) [16].
Statistical analysis
Data are presented as mean±standard deviation for continuous variables and as frequencies and percentages for categorical variables. The Fisher’s exact test or the unpaired t-test was used to assess categorical and continuous variables, respectively. The cutoff value of the number of DWI-positive lesions for predicting SIC was obtained using the receiver operating characteristic (ROC) curve. Statistical analysis was performed using R version 4.0.5, and correlation matrices were displayed using the R language program package.
RESULTS
Endovascular treatments were performed for 60 unruptured aneurysms in 53 patients and 30 patients with a ruptured aneurysm. Fifty-five patients (68.7%) were female, and the mean age was 62.3, ranging from 37 to 87 years.
Table 1 presents a comparison between patients with ruptured and unruptured aneurysms. There were no significant differences in the sex or risk factors for atherosclerosis. The ruptured aneurysms were significantly larger than the unruptured aneurysms (6.7±2.5 mm vs. 5.3±1.9 mm, p=0.004). Stent use was significantly more frequent in patients with unruptured aneurysms than in those with ruptured aneurysms (69.8% vs. 36.7%, p=0.007).
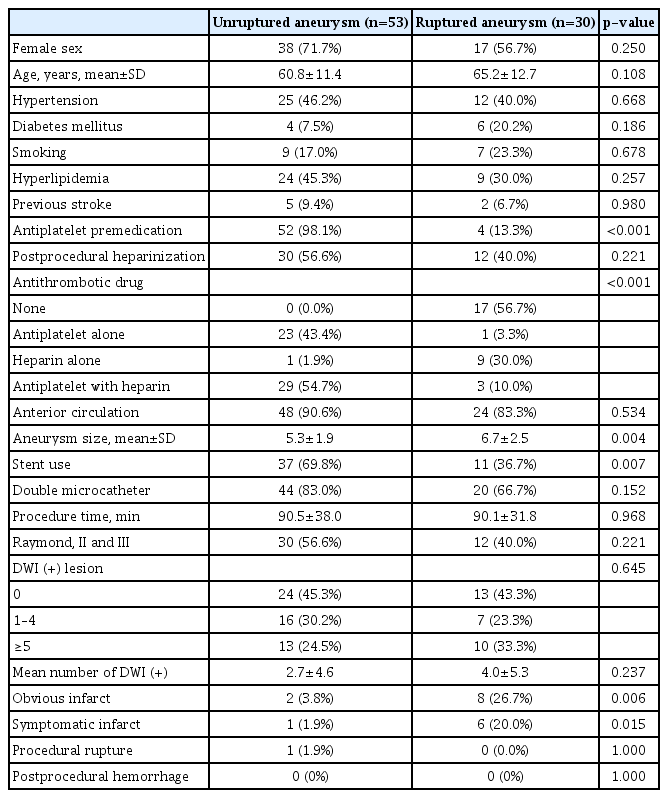
Comparison of baseline demographics, anti-thrombotic drugs, clinical outcomes, and postprocedural DWI-positive lesions between unruptured and ruptured aneurysms
According to the aneurysm rupture state, antithrombotic drugs were administered differently between patients with ruptured and unruptured aneurysms (Table 1). Twenty-six patients with ruptured aneurysms (86.7%) did not receive any antithrombotic drugs (n=17, 56.7%) or only underwent postprocedural heparinization (n=9, 30%). In contrast, 52 patients with unruptured aneurysms (98.1%) were administered dual antiplatelet premedication alone (n=23, 43.4%) or antiplatelet premedication with postprocedural heparinization (n=29, 54.7%).
The overall rate of DWI-positive lesions was 55.4% (n=46). There were no significant differences in the occurrence rate (45.3% vs. 43.3%, p=1.000) and the number of DWI-positive lesions (2.7±4.6 vs. 4.0±5.3, p=0.237) between patients with unruptured and ruptured aneurysms. SIC occurred in seven patients (8.4%), and all SICs occurred in patients with obvious infarcts. SIC occurred more frequently in patients with ruptured aneurysms than in those with unruptured aneurysms (1/53 [1.9%] vs. 6/30 [20.0%], p=0.015). The incidence of SIC was significantly higher in patients without antithrombotic drugs than in those with antithrombotic drugs (5/17 [29.4%] vs. 2/66 [3.0%], p=0.003). The incidence of SIC did not differ between patients with stent and those without stent (3/48 [6.25%] vs. 4/35 [11.4%], p=0.661).
Symptoms of SIC were as follows: monoparesis (n=1), hemiparesis (n=4), dysarthria (n=1) and aphasia (n=1). The day of symptom developed was as follows: the day of procedure (n=4), the second day after the procedure (n=2), and the 5th day after the procedure (n=1). The 3-month mRS scores of the seven patients were 1 (n=4), 2 (n=2), and 3 (n=1).
The ROC curve analysis showed that the cutoff value of DWI-positive lesions for predicting SIC was 5 (area under the curve, 0.951; sensitivity, 100%; specificity, 78.9%; p<0.001). DWI-positive lesions ≥5 were observed in 23 patients (27.7%). The number of DWI-positive lesions was significantly more prominent in the SIC group than in the asymptomatic one (11.9±4.3 vs. 2.4±4.1, p<0.001). Patients with DWI-positive lesions <5 were more frequently observed in the postprocedural heparinization group than in the no postprocedural heparinization group (36/42 [85.7%] vs. 24/41 [58.5%], p=0.012).
When divided into two groups according to the cutoff value, there was a significant difference in the use of antithrombotic drugs and procedure time (Table 2). The procedure time was significantly longer in the group with ≥5 DWI-positive lesions (p=0.030). Obvious infarct and SIC occurred significantly higher in the DWI (+) ≥5 than in those with DWI (+) <5 (p<0.001).

Comparison of risk factors for thromboembolic complications between DWI-positive lesion <5 and ≥5 groups
Patients with postprocedural heparinization had significantly fewer DWI-positive lesions than those without postprocedural heparinization (1.8±2.8 vs. 4.5±6.1, p=0.013). Patients with postprocedural heparization had a lower incidence of SIC than those without postprocedural heparinization (1/42 [2.4%] vs. 6/41 [14.6%]), however, the significance was not enough (p=0.107). In patients with ruptured aneurysms (n=30), twelve patients received postprocedural heparinization, and eighteen patients did not receive postprocedural heparization. Of them, six patients experienced SIC (20.0%), including one patient in the postprocedural heparinization group and five patients in the no postprocedural heparinization group (1/12 [8.33%] vs. 5/18 [27.8%], p=0.402).
Seventeen patients with ruptured aneurysms (56.6%) underwent postprocedural surgery, including EVD (n=8), lumbar drainage (n=9), and ventriculoperitoneal shunt placement (n=2). Of the 12 patients with ruptured aneurysms who underwent postprocedural heparinization, 9 underwent lumbar drainage without complications, and 3 did not undergo any other surgery. EVD-related focal hemorrhage occurred in two patients, and none of them received antithrombotic drugs. There were no cases of HIT.
DISCUSSION
Clinically silent infarcts following endovascular procedures remain relatively common despite the increasing experience with endovascular techniques and routine use of antithrombotic drugs. However, the clinical significance and long-term effects of these events are controversial and debatable. There is increasing evidence that the cumulative burden of ischemic brain injury might cause cognitive decline or neurological deficits [9,23]. Studies from cardiac and orthopedic literature have also found that DWI lesions after procedures have reduced cognitive function on neuropsychological examinations [4,12].
A systematic review reported that one out of two patients had infarcts on DWI following endovascular treatment of intracranial aneurysms [1]. Consistent with this study, DWI-positive lesions occurred in 55.4% of the patients in our study. Previous studies demonstrated that risk factors for DWI-positive lesions were stent-assisted coiling, larger aneurysm size, incomplete occlusion, old age, and procedure time [7,15,21]. In this study, longer procedural time showed a positive association between endovascular treatment and postprocedural DWI-positive lesions.
Kang et al. reported that the cutoff value of DWI-positive lesions for predicting SIC was ≥6, and there were significantly more DWI-positive lesions in the SIC group than in the asymptomatic group [10]. Similar to their study, the cutoff value of DWI-positive lesions for predicting SIC was ≥5 in our study. However, SIC was not associated with dot-like lesions but with obvious infarcts greater than 10 mm on DWI. Our results showed that all patients who developed obvious infarcts had five or more DWI-positive lesions. Our study suggests that the size of DWI-positive lesions and the number of lesions also had a significant relationship with the SIC.
The optimal antiplatelet preparation for preventing thromboembolic and hemorrhagic complications in the endovascular treatment of ruptured aneurysms remains controversial. Several studies have found that preprocedural antiplatelet medication does not improve outcomes in patients with ruptured aneurysms [2,22]. This study showed no significant difference in the incidence of DWI-positive lesions between patients with ruptured aneurysms and those with unruptured aneurysms despite the absence of antiplatelet preparation in patients with ruptured aneurysms. Our results also showed that SIC occurred more frequently in patients with ruptured aneurysms than in patients with unruptured aneurysms. However, SIC occurred less frequently in patients with ruptured aneurysms who underwent postprocedural heparinization than in those with ruptured aneurysms who did not. This result suggests that postprocedural heparinization in patients with ruptured aneurysms may reduce the risk of DWI-positive lesions and SIC. Our results showed that most SICs occurred within two days after the procedure, which may suggest the effectiveness of postprocedural heparinization for 24 hours after the procedure.
Heparin is widely used to prevent or treat thromboembolism; however, concerns about hemorrhagic complications limit its use in patients with ruptured aneurysms. Previous studies have demonstrated that intravenous heparin infusion is safe in the setting of aneurysmal SAH after securing the aneurysm [3,19,25]. Our findings also show that heparin infusion effectively prevents embolism in patients with ruptured aneurysms, with no increased risk of hemorrhagic or HIT complications. Heparin is the most negatively charged molecule and has various effects, including anti-inflammatory effects [13,14,20]. Recent studies have suggested that heparin infusion reduces delayed neurological deficits, cognitive dysfunction, and severe cerebral vasospasm [8,11].
This study has several limitations. First, it is a retrospective, single-center study with a small sample size. There is a potential bias in the selection of patients who underwent postprocedural heparinization and DWI. Second, some DWI abnormalities were difficult to distinguish, and a perfect consensus was not always achieved. Third, we did not consider cognitive dysfunction for checking neurologic status. Previous studies reported that cognitive deficits could occur after endovascular treatment for cerebral aneurysms, although neurological deficits did not occur. Fourth, our study did not include cases of late thromboembolism. We focused only on the analysis of acute perioperative DWI-positive lesions within 48 hours following the procedure. Finally, it may be necessary to compare magnetic resonance imaging (MRI) immediately after the procedure with MRI within 48 hours after the procedure to prove the effectiveness of postprocedural heparinization. However, in this study, there was no MRI immediately after the procedure. Most MRIs were taken between 24 and 48 hours after the procedures. Further studies comparing MRI immediately after the procedure with MRI within 48 hours after the procedure are needed to confirm these preliminary results.
CONCLUSIONS
The incidence of DWI-positive lesions following endovascular treatment did not differ significantly between the ruptured and unruptured aneurysms. However, SIC occurs more frequently in patients with ruptured aneurysms. Postprocedural heparinization effectively reduced the number of DWI-positive lesions following endovascular treatment without complications, and it also tended to reduce the incidence of SIC after the procedures. Further studies with larger sample size are needed to confirm these preliminary results.
Notes
Disclosure
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.