Incomplete Clipping Resulting from Scissoring of the Clip Blades during Treatment of a Large Atheromatous Aneurysm
Article information

Abstract
The cerebral aneurysm 'clip scissoring' phenomenon resulting from clip blade twisting is an unpredictable surgical complication. Additionally, incomplete clipping resulting from the presence of an atherosclerotic wall in the neck of the aneurysm can also cause unforeseen problems. Here, the authors present an unusual case of incomplete clipping of a large, atheromatous aneurysm resulting from clip scissoring, which was treated with additional endovascular coiling.
INTRODUCTION
When considering long-term patient outcomes, direct clipping of the aneurysm neck is a still an effective and reliable technique, especially when treating a large, complex aneurysm. However, as surgical tools are now made primarily from a titanium alloy, there have been some reports of a scissor-like deformation when using relatively long and straight/bayonet clips made of titanium.1)2)3)4) The 'clip scissoring' phenomenon refers to twisting of the clip blades, and is likely to be associated with potentially devastating complications. Previous reports describing complications arising from direct clipping of the atherosclerotic or calcified wall of the neck have focused on ischemic cerebrovascular events,5) but incomplete clipping has not been notably discussed before. In this report, we present a case of incomplete clipping of a large, atheromatous aneurysm, resulting from the clip scissoring phenomenon, and discuss the subsequent pathophysiologic implications.
CASE REPORT
A 59-year-old female patient with a history of hypertension was referred to our department for a large right middle cerebral artery (MCA) aneurysm, which was incidentally discovered in a magnetic resonance angiography (MRA) test during routine health screening. MRA revealed a large right MCA aneurysm with a maximum diameter of 19.5 mm and a neck diameter of 11.6 mm (Fig. 1A, B). Cerebral angiography confirmed the presence of the MCA aneurysm and provided more detailed anatomical and structural information (Fig. 1C, D and E).
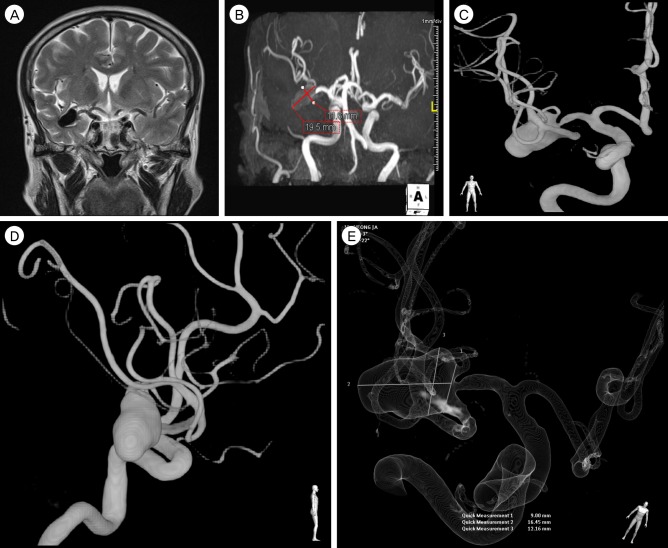
T2-weighted coronal magnetic resonance imaging (MRI) (A) and magnetic resonance angiography (MRA) (B) performed during a health-screening test demonstrating a large, unruptured middle cerebral artery aneurysm. Reconstruction of 3D rotational angiogram with the anterioposterior (C), and lateral (D) view, and translucent 3D rotational image (E) providing more detailed structural information including the precise size of the aneurysm.
Because the aneurysm had a wide neck, microsurgical exploration and clipping, rather than coil embolization, was planned. At the time of surgical exploration, atheromatous changes encompassed the parent artery and aneurysm neck, and extended further into the sac. Furthermore, differently from the usual unruptured aneurysm, a large aneurysm sac was protruding into the normal brain parenchyma. To avoid unnecessary brain injury, only the aneurysm neck was exposed and dissected. Clipping was achieved using a titanium straight 200 mm clip (model FT790D; Aesculap Instruments Corp., Tuttlingen, Germany). After confirming that the clip blade had reached the far side of aneurysm neck, the surgery was completed, and the patient awoke without deficit (Fig. 2). However, a post-operative 3-dimensional computed tomography angiogram (3D-CTA) demonstrated significant filling of the aneurysm, which had diminished slightly in size (Fig. 3A, B). Subsequent cerebral 3D rotational angiography confirmed scissoring of the clip blade on the aneurysm neck, rendering the clipping incomplete, and allowing the aneurysm to fill with blood (Fig. 3C, D and E). Since the aneurysm neck had narrowed as much as a microcatheter could insert, additional endovascular coiling treatment for the residual aneurysm was performed, and complete obliteration of the residual aneurysm was documented (Fig. 4).
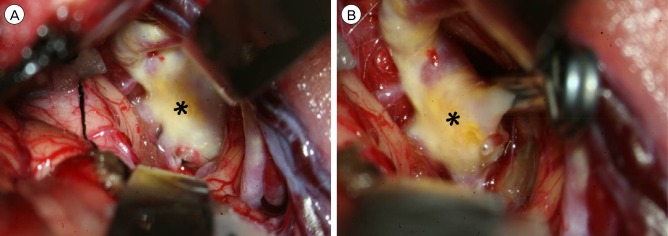
Intraoperative photographs during neck clipping surgery showing the right middle cerebral artery aneurysm before (A) and after (B) clipping using a 20 mm straight clip. Note that atherosclerotic changes (asterisk) encompassing the parent artery, aneurysm neck, and extending further into the aneurysm sac. Clip blades seem to be closed without any perceivable distortion as viewed from the operative field.
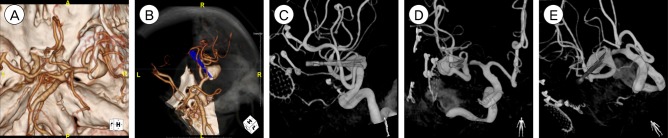
Post-operative 3-dimensional computed tomography angiogram (3D-CTA) revealing significant filling of the aneurysm (A, B). Subsequent cerebral 3D rotational angiography (C, D and E) showing scissoring of the clip blade onto the aneurysm neck and incomplete clip closure, which allowing the aneurysm to be filled with blood.
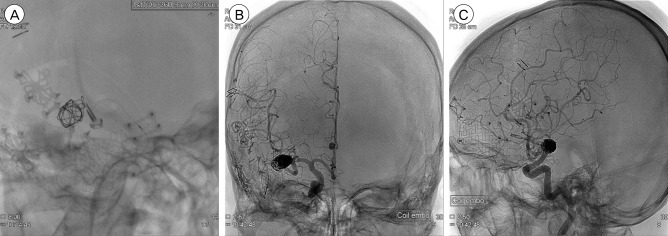
Neurointerventional image during coil embolization showing the microcatheter barely entering the aneurysm (A). Post-treatment non-subtracted angiogram showing no contrast filling of the aneurysm (B, C).
The Patient made an uncomplicated recovery for both clipping and coil embolization and underwent an uneventful clinical follow-up for more than 2 year.
DISCUSSION
Clip scissoring is reported to occur when an aneurysm is particularly large, containing calcification, a broad neck, mural thrombus, or an atherosclerotic neck.3) It is most devastating when the scissoring results in damage to the aneurysm neck, which has been linked to rupture during clip manipulation. When accompanied by atherosclerotic changes, scissoring might disturb blood flow by parent artery stenosis or occlusion, resulting from clip slippage following scissoring due to clip closing interference by an atheroma.7)
Although the authors of a few studies have described other difficulties in obliteration of atherosclerotic aneurysms using a clip, there are few reports in incomplete obliteration of an aneurysm following clipping in the literature. This phenomenon is believed to be incomplete closure of the clip blade due to irregularly distributed atheromas within the neck when an aneurysm is large and have a broad neck. It is difficult to achieve the force necessary to occlude an aneurysm through clipping, being hindered by hard, intermittently spaced plaques such as atheromas, which may subsequently lead to an incomplete closure of the clip blade and slipping of the clip. Schematic drawings representing these findings are presented in Fig. 5.
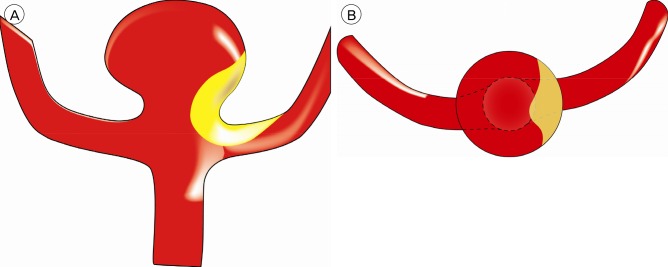
Illustrations showing the scissoring of the clip and incomplete clipping resulting from the presence of an atherosclerotic wall in the neck of the aneurysm. (A) Lateral view of the aneurysm containing atheroma within the neck. (B) Axial view severed just above the neck of the aneurysm. (C) When the neck of the aneurysm is clipped with a long clip made of titanium, scissoring phenomenon may occur due to interference of atheroma. (D) Axial view of incomplete closure of the clip blade resulting from irregularly distributed atheroma within the neck. Note that blood flow is still maintained through remaining neck of the aneurysm.
In our patient, the incomplete clipping and the scissoring of the clip was not detected in the operative field due to limited exposure of the aneurysm and its neck. Although sufficient dissection and exposure of the aneurysm is necessary to successfully apply an aneurysm clip, there could be unwanted injury of normal brain tissue and increased risk of rupture during dissection, especially when the aneurysm is large and protruding into the parenchyma. A second surgical attempt may be performed to obtain complete occlusion and correct the scissoring of the clip; it might not avoid an unwanted brain injury under the same circumstance. Because the aneurysm neck was narrowed by the incomplete clipping, additional endovascular coiling was performed and the remaining aneurysm was successfully occluded.
When considering this case in light of the previous reports, the conditions in which clip scissoring and incomplete clipping occur are: 1) the aneurysm is large and has a broad neck with atherosclerotic changes;1)2) 2) the clips used in this case and other reports where the clipping problems occurred were the straight or bayonet type with a longer than 15 mm blade length, made of pure titanium or a titanium alloy.1)2)6)
We believe that preoperative planning should take complete account of aneurysm morphology as well as all factors that may affect patient outcomes. Unfortunately, some important findings such as the presence of atherosclerosis in the aneurysm neck, a pinched aneurysm sac protruding into the parenchyma, scissoring or incomplete closure of the clip, cannot be easily predicted. Under these circumstances, particularly when treating unruptured aneurysms, it is imperative to avoid complications.
Considering those unpredictable situations, the authors conclude that when possible the surgeon could avoid complications by adhering to the following rules. 1) Expose the aneurysm as much as possible so that the opposite side of the aneurysm neck and relevant parent artery can be seen. 2) Re-adjust the clip with extreme care to avoid damage to the aneurysm neck when scissoring is noticed. 3) If the first clip fails to close completely due to atheroma within the aneurysm neck, mount an additional clip parallel to the first on the distal portion of the aneurysm while ensuring blood flow is preserved in the parent artery. 4) If clip scissoring or incomplete closure of the clip is not perceived in the operative field and profound filling of the aneurysm is observed during a post-operative radiologic examination, the use of coil embolization as a means of alternative treatment is preferable.
CONCLUSION
We describe incomplete clipping resulting from scissoring of the clip blades during treatment of a large atheromatous aneurysm. The present case emphasize that in treating a large aneurysm having a broad neck in which considerable atheroma reside, complete exposure of aneurysm with fine dissection should be preceded before attempting clip mounting, and ,once clip was mounted, reexamination of aneurysm status including aneurysm sac and neck, parent artery, clip blade alignment is crucial for the completeness of aneurysm obliteration.
Notes
Disclosure: The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.