



INTRODUCTION
Hemangioblastomas are highly vascularized central nervous system (CNS) neoplasms with a predilection for the cerebellum, brainstem, and spinal cord.1) Clinical presentation typically occurs in the fifth decade for sporadic cases and as early as the third decade for patients with a diagnosis of von Hippel-Lindau (VHL) disease.7)20) These tumors are rarely found in children.3) Symptoms correlate with regional compression of cerebrospinal fluid (CSF) flow or eloquent tissue and can include cerebellar signs and symptoms, cranial nerve deficits and weakness and spasticity, among other findings. Despite extensive literature describing the diagnosis, treatment, and prognosis of these lesions,6) individual cases still present a surgical quandary given their frequently eloquent location and high degree of vascularity. We report on a case of a young female with focal posterior fossa hemorrhage from an unknown vascular lesion. We detail our surgical management in the context of similarly rare cases.
CASE REPORT
The patient was a 23 year-old female with no known medical history presenting with a Glasgow Coma Score (GCS) of 3 and reactive pupils after being found down without signs of head trauma or intoxication. A non-contrast head computed tomography (CT) scan showed a subarachnoid hemorrhage (SAH) in the posterior fossa (Fig. 1A) with extension into the third, fourth, and lateral ventricles (Fig. 1B). A 2 cm vascular lesion below the cerebellar margin was observed following contrast administration (Fig. 1C). An external ventricular drain (EVD) was inserted into the right frontal horn of the lateral ventricle to relieve early hydrocephalus (level set at 20 cm H2O with clear CSF return), and a diagnostic cerebral angiogram was planned. However, less than one hour following ventriculostomy placement, acute hemorrhage was observed within the EVD tubing, and intracranial pressures (ICP) rose beyond 100 cm H2O. The patient was taken to the operating room emergently for posterior fossa decompression. Intraoperatively, following a wide suboccipital craniectomy, C1 laminectomy, and posterior fossa dural opening, a firm, well-circumscribed, highly vascular mass was found below the obex at the craniocervical junction. Manipulation of the mass led to brisk hemorrhage and attempts to dissect circumferentially around the mass were limited due to significant swelling of the cerebellar hemispheres. Given the primary objective of posterior fossa decompression and the unclear anatomy of the lesion, the decision was made to stage the operation after performance of magnetic resonance imaging (MRI) and angiography in order to further characterize the lesion.
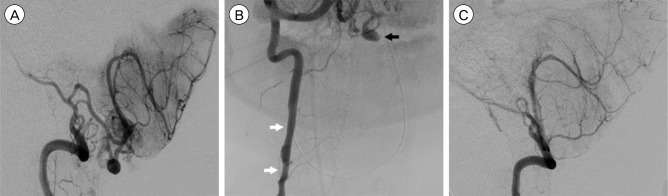
Interval MRI showed a homogeneously enhancing, dorsal exophytic mass at the medullary-cervical junction (Fig. 1D). T2-weighted imaging showed numerous, large flow voids and an abnormal cord signal throughout the cervico-medullary junction, without evidence of syrinx formation. A four-vessel catheter angiogram confirmed a hypervascular mass centered at the foramen magnum, compressing the posterior medulla, and supplied by an enlarged posterior meningeal artery (PMA) branching from the right proximal intradural vertebral artery segment. The tumor was also supplied by the contralateral PMA and collateral branches off the ipsilateral posterior inferior cerebellar artery (PICA). A 4.5 mm fusiform aneurysm of the right PMA branch was embedded within the mass (Fig. 2A). In addition, multiple dissections were observed in the cervical segment of the right vertebral artery (Fig. 2B). Transarterial embolization of the right PMA was unsuccessful, as no branch could be safely catheterized and potentially occluded without risking the blood supply to the brainstem or cerebellum.
The patient returned to the operating room two days later for definitive tumor resection and aneurysm clipping. A right far lateral approach was utilized in order to obtain proximal control of the right vertebral artery. The cerebellar hemispheres remained swollen, preventing circumferential dissection of the tumor despite additional bone resection and CSF drainage. Clip placement did not reduce tumor vascularity; therefore, feeding vessels on the tumor surface were coagulated and disconnected. As the tumor was internally debulked, the collapsed right PMA aneurysm was visualized in the anterior and inferior capsule wall of the tumor. The aneurysm wall was separated from the tumor capsule, so that it was trapped and removed along with all visible tumor. Postoperative imaging showed no residual evidence of aneurysm or tumor (Fig. 2C). Pathologic review of the surgical tumor specimen was diagnostic of hemangioblastoma, WHO grade I (Fig. 3). Post-operatively the patient transiently displayed finger and proximal extremity movement to command. However, she returned to a comatose state and thereafter remained EVD-dependent. After two months of little clinical improvement, she was transitioned to comfort care at her family's request. She expired on post-operative day 53. No autopsy or further testing for VHL was performed.
DISCUSSION
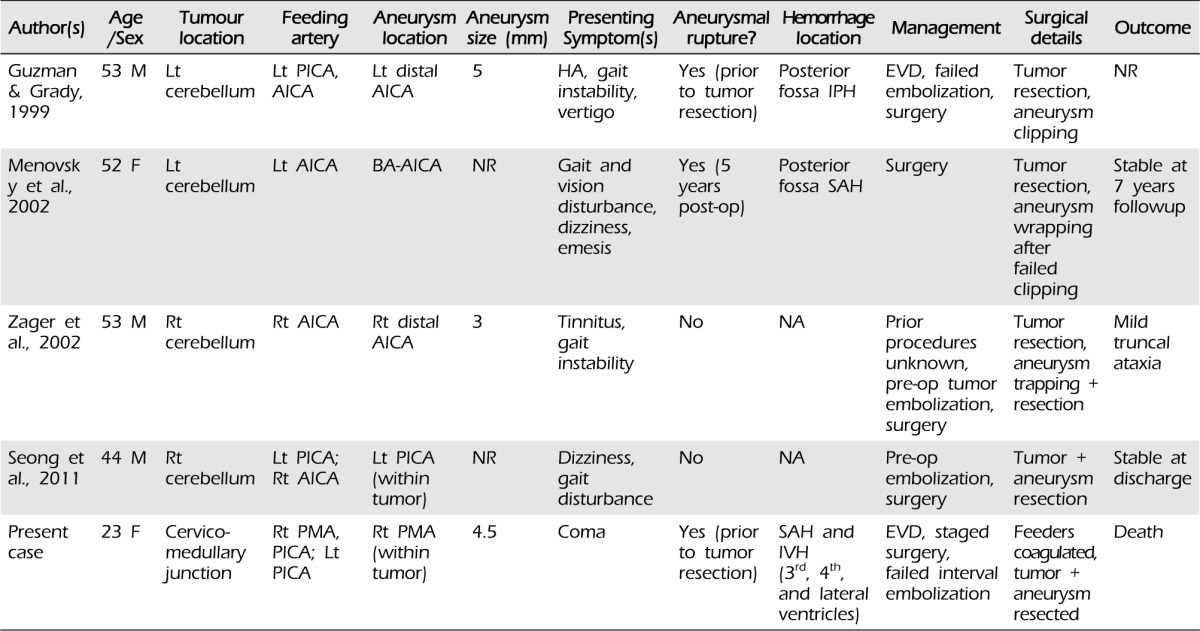
Hemangioblastoma associated with a coexisting feeding artery aneurysm is extremely rare (Table 1).11)12)17)21) One report described an aneurysm directly embedded within the tumor capsule, similar to our case.17) In addition, although two cases have been associated with aneurysm rupture,11)12) only one occurred prior to tumor removal.11) The case presented here is the first in which coma was the presenting symptom and acute re-hemorrhage compounded the surgical complexity of the case.
Aneurysms of the posterior circulation are less common than those of the anterior circulation, and involvement of the posterior meningeal artery is even more unusual. Previous reports have implicated trauma, anomalous origin from PICA, dural arteriovenous fistula, and PICA thrombosis leading to collateralized PMA as causes of true PMA aneurysms and pseudoaneurysms.2)4)10)14)16) In general, the etiology of fusiform aneurysms is also poorly understood, although numerous causes, including atherosclerosis and dissection, have been proposed.8) To the best of our knowledge, this is the first reported case of a fusiform PMA aneurysm associated with a brain tumor. The patient's tumor was supplied not only by the right PMA but also by collaterals from the ipsilateral PICA and contralateral PMA, consistent with previous reports of congenital and acquired PMA-PICA collateralization.4)15)18)19) In this way, increased hemodynamic flow from collaterals and associated wall shear stress may have contributed to this patient's multiple posterior circulation dissections and, possibly, formation of the hemangioblastoma-fusiform PMA aneurysm complex.
The successful approach to and removal of tumor-aneurysm complexes benefit from preoperative planning in a number of ways. First, preoperative embolization can be performed prior to surgery to reduce intraoperative bleeding. Embolization via particles is safe and effective but is associated with higher rates of post-embolization hemorrhage in cerebellar compared to spinal cord masses (50% vs. 5%, respectively) because larger capillary diameters in cerebellar hemangioblastomas allow entry of small particles, which occlude the venous network, leading to retrograde hypertension.5)13)17) This risk is minimized with use of liquid agents, which penetrate deep into the capillary bed of the tumor without entering the venous compartment.9)17) Occasionally, however, embolization is not possible due to the tortuosity of the vessel involved,11) or, as with our patient, due to concerns for perfusion to other vital structures.
Second, the surgical approach can be carefully designed to achieve both tumor resection and decompression of the vascular lesion. In this case, the bilateral suboccipital craniectomy and C1 laminectomy were required for posterior fossa decompression, and ultimately this approach would likely have been sufficient for tumor resection. However, proximal control of the right vertebral artery would still have required skeletonization of the vertebral artery via a far lateral approach (i.e., widening of the foramen magnum and partial condylectomy), which we believe could be achieved in a single stage. Thus, although the active bleeding within hours of presentation did not permit performance of an initial angiogram, staging the procedure allowed for further diagnostic workup, and redirection of our approach, and allowed us to achieve definitive resection of both the aneurysm and tumor.
Finally, a case can be argued for no intervention at all, given the patient's poor presentation and eventual grave prognosis. However, we felt that, given the acuity of her symptoms and her young age, she might possess enough physiological reserve to overcome her brainstem injury.
CONCLUSION
We report on the occurrence of a fusiform posterior meningeal artery aneurysm embedded within a dorsal exophytic brainstem hemangioblastoma. Although the etiology of this association is not completely understood, it is likely that the combination of histopathological features and hemodynamic properties brought these two entities in conjunction. Our experience with this complex case confirms the importance of early diagnosis and intervention with special consideration of available treatment options once the acute phase of the disease has been addressed.


 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






