Endovascular Coil Embolization After Clipping: Endovascular Treatment of Incompletely Clipped or Recurred Cerebral Aneurysms
Article information

Abstract
Objective
The presence of a cerebral aneurysm remnant after surgical clipping is associated with a risk of regrowth or rupture. For these recurred aneurysms, coil embolization can be considered as a treatment option. We retrospectively reviewed cases of ruptured or regrown aneurysms after clipping treated by endovascular coil embolization.
Materials and Methods
We conducted a retrospective review of patients with ruptured or recurred aneurysm after clipping, who underwent coil embolization between January 1995 and December 2013. We evaluated clinical information and the outcomes of these cases.
Results
Eight patients were treated by endovascular coil embolization after surgical clipping. Six aneurysms were located in the anterior communicating artery, one in the posterior communicating artery, and one in the middle cerebral artery bifurcation. All patients were initially treated by surgical clipping because of a ruptured aneurysm. Aneurysm recurrence at the initial clipping site was detected in all cases. The median interval from initial to second presentation was 42 months. In four patients, aneurysms were detected before rupture and the four remaining patients presented with recurrent subarachnoid hemorrhage. All patients were treated by coil embolization and showed successful occlusion of aneurysms without complications.
Conclusion
Endovascular coil embolization can be a safe and successful treatment option for recurred aneurysms after clipping.
INTRODUCTION
The main goal in treatment of cerebral aneurysms is complete obliteration of the aneurysmal sac and neck. Surgical clipping is a successful treatment option for achievement of this goal. However, remnant aneurysm is observed on follow-up angiography after surgical clipping in 1.6 to 14.9% of cases, and the risk of rebleeding from these remnant aneurysms is 4 to 14.7%.1)2)3)4)5)6)10)11)12) These lesions can result in regrowth or rupture after months or years, with potential for serious and fatal consequences. Thus, treatment should be considered when recurred or regrown aneurysms are identified. Until now, endovascular coil embolization, surgical clipping, or their combination was performed for treatment of these lesions.7)9) However, second surgical clipping is technically difficult and a burden for neurosurgeons because of surgical site adhesions or risk of failure.5) In addition, patients may not be medically stable enough to undergo a second craniotomy or may refuse the procedure. Thus, endovascular coil embolization has been considered as a treatment option for postoperative aneurysm remnant or recurrence.4)5)6)11)12)13)
Here, we report on our experience using endovascular coil embolization for treatment of aneurysm remnant or recurrence after surgical clipping.
MATERIALS AND METHODS
Patients
We collected information on patients who underwent endovascular coil embolization for aneurysm remnant or recurrence after surgical clipping at our institution between 1995 and 2013. We collected data regarding age at the time of second treatment, sex, initial clinical presentation at the time of clipping, initial aneurysm size, aneurysm location, reason for second treatment, size of the aneurysm at second treatment, degree of occlusion after coil embolization, procedural-related complications, follow-up angiography and follow-up clinical status using the Glasgow outcome scale (GOS).
Follow-up protocol after clipping
We performed postoperative angiography using computed tomographic (CT) angiography two weeks after clipping. If the patient showed symptoms related to rebleeding, immediate evaluation was performed. After discharge, if evidence of aneurysm remnant was observed on postoperative angiography, annual follow-up using CT angiography was performed. For the patient without aneurysm remnant, we performed follow-up CT angiography five years after initial treatment.
Second treatment indication for aneurysm remnant or recurrence and endovascular procedure
The second treatment was administered for the recurrent aneurysm leading to subarachnoid hemorrhage (SAH) and the aneurysm remnant showing gradual growth on follow-up angiogram. In addition, treatment was also administered for considerable aneurysm remnant after incomplete clipping on postoperative angiogram. All patients were treated with an endovascular procedure by experienced neurosurgeons or neuroradiologists.
Coil embolization was performed under general anesthesia using a biplane C-arm angiographic system. For unruptured aneurysms, antiplatelet drugs were administered for one week before the procedure. A bolus of 3,000 U heparin was administered after femoral arterial sheath placement. Intermittent boluses of 1,000 U/hr heparin were then administered. Antiplatelet preparation and intra-procedural anticoagulation were not used in cases of ruptured aneurysms. Immediate post-embolization angiography was performed in all patients and the angiographic results were reported using the Raymond scale.
RESULTS
Eight patients, five females and three males, were treated by endovascular coil embolization after surgical clipping. The median age at the time of coiling was 61.5 years (range, 39-69). All patients were all initially treated by surgical clipping due to ruptured cerebral aneurysms. A summary of the clinical and radiological data is shown in Table 1. Six aneurysms were located in the anterior communicating artery (ACoA, 75%), one in the posterior communicating artery (PCoA), and one in the middle cerebral artery bifurcation (MCAB). The median aneurysm size at the first presentation was 7.2 mm (range, 3-11.5 mm). All cases initially resulted in complete clipping of the aneurysmal neck, except one patient (case 8, intended remnant due to technical difficulty). The interval between the initial and second treatment was from two weeks to 19 years. Of eight patients, three patients underwent additional endovascular coil embolization within one month after clipping.
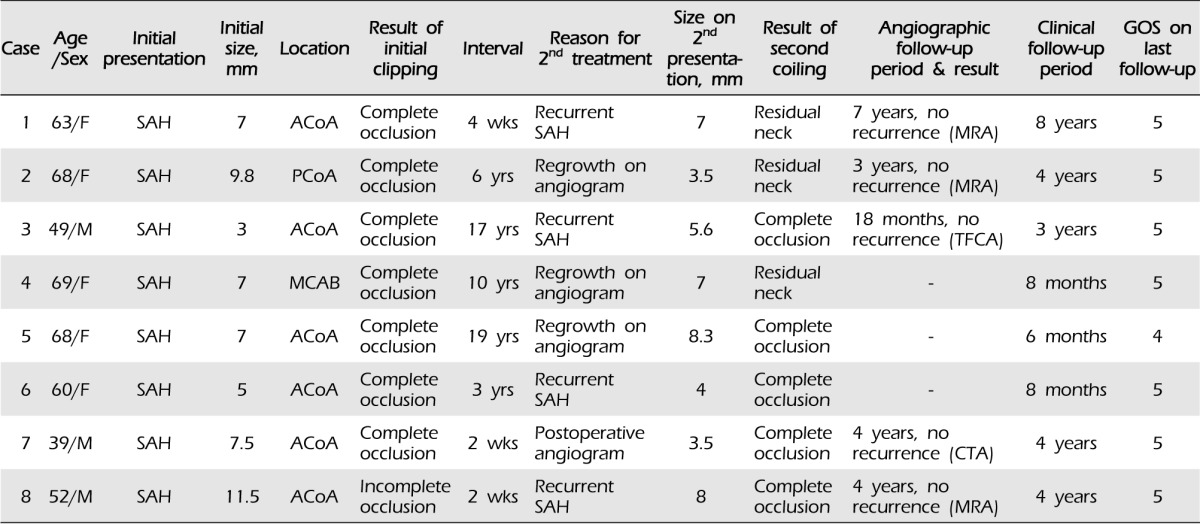
Summary of clinical and angiographic data of the patients
The reasons for the second treatment were recurrent SAH from recurred aneurysm in four cases and aneurysm recurrence was detected on a follow-up angiogram in four cases. The median size of the aneurysms at the time of coiling was 6.3 mm (range, 3.5-8.3 mm). In coil embolization for the second treatment, complete occlusion was achieved in five patients and minimal residual neck was observed in the three remaining patients. No procedural-related complications occurred during or after coil embolization.
A follow-up angiogram was performed in five patients and no additional aneurysm recurrences were found (median follow-up time, 48 months). Three patients had no data due to a short follow-up period. We obtained clinical follow-up data on all patients (median follow-up period, 42 months). Seven patients showed no functional impairment (GOS 5) during the follow-up period. One patient showed slight functional impairment (GOS 4) due to a thalamic hemorrhage during the follow-up period (case 5).
Case illustrations
Case 1: 63-year-old woman, ACoA aneurysm
A 63-year-old woman visited the emergency room with a sudden severe headache. She was diagnosed with Hunt-Hess grade II SAH. Digital subtraction cerebral angiography was performed and showed an aneurysm measuring 7.0×4.0 mm in size on the ACoA (Fig. 1A). Surgery was performed and resulted in complete clipping of the aneurysmal neck. After the surgical clipping, she was alert and recovered without any neurological deficit. However, she complained of a sudden recurrence of severe headache four weeks after clipping, and brain CT showed recurrent SAH. We immediately performed cerebral angiography, and contrast filling in the aneurysmal sac was detected (Fig. 1B). Endovascular coil embolization was performed using the single catheter technique without occurrence of procedural-related complications (Fig. 1C).

(A) Left carotid angiogram showing a 7 mm sized ruptured anterior communicating artery aneurysm. (B) Postoperative follow-up angiogram shows 7 mm sized recurred aneurysm due to incomplete clipping. (C) Coil embolization for recurred aneurysm.
Case 4: 69-year-old woman, MCAB aneurysm
A 69-year-old woman visited the outpatient clinic with a mild headache. She had a history of SAH due to a ruptured middle cerebral artery bifurcation (MCAB) aneurysm and had undergone surgical clipping in our institution 10 years before this visit. She was lost to follow-up three years after clipping. Recurrence of the aneurysm at the same site was detected on cerebral angiography CT. Regrowth of the aneurysm was detected on digital subtraction cerebral angiography (Fig. 2A). Endovascular coil embolization using the double catheter technique was performed successfully without complication, although a minimal residual sac was noted (Fig. 2B).
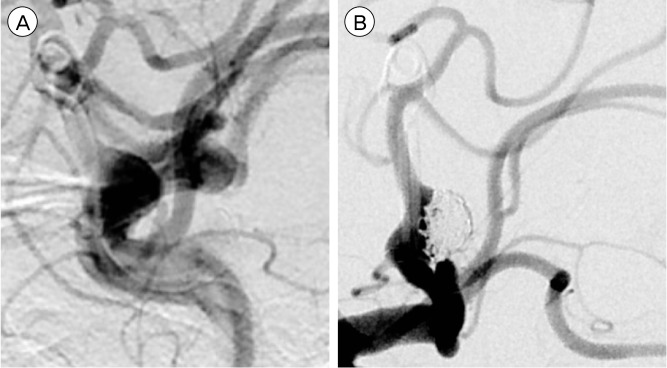
(A) Aneurysm regrowth in the middle cerebral artery bifurcation. (B) Coil embolization for aneurysm regrowth.
DISCUSSION
In treatment of cerebral aneurysm, the main goal is to occlude the aneurysmal neck in order to reduce the possibility of bleeding. Successful occlusion can be achieved by surgical clipping or endovascular coil embolization. However, even after complete occlusion of an aneurysm, a recurrent aneurysm, a residual neck, de novo aneurysm formation, and a slipped clip can be detected on follow-up angiographic studies.3)4)5) According to the International subarachnoid aneurysm trial (ISAT) reported in 2002,7) the risk of rebleeding from the ruptured aneurysm after one year was zero per 1081 patient-years for patients who underwent neurosurgical clipping. However, in longer follow-up of ISAT patients, Campi et al.1) reported that after surgical clipping, among 1012 patients, retreatment ws performed in 39 patients (3.8%) and the mean time to retreatment was 5.7 months. Tsutsumi et al.14) reported that the cumulative recurrence rate of SAH after complete obliteration of an aneurysm is 2.2% at 10 yrs and 9.0% at 20 yrs after the original treatment. These recurred SAH can be serious and sometimes fatal.2)3)4)5)6) Drake et al.4) reported that if a remnant cerebral aneurysm is detected, there is a high probability of hemorrhage and second treatment is required. Recurrence of aneurysms 20 yrs after the first treatment has been reported and similarly, in our study, three cases were detected within one month and the other three cases were detected 10 yrs after the first treatment (10, 17, and 19 yrs).13) For this reason, all neurosurgeons recognize the necessity of periodic angiographic follow-up. However, there are no approved guidelines. Tsutsumi et al.14) reported that more frequent follow-up angiography (e.g., every 3 yrs) may be indicated for patients with incompletely clipped aneurysms. Wermer et al.15) recommended follow-up every five years, particularly in young women with SAH. Accordingly, continuous long-term follow-up would be necessary even in aneurysms treated with clipping.
Before development of coil embolization, re-operation for a recurred or regrown aneurysm was the only option for treatment. However, the second clipping is usually more difficult due to changes in the anatomical structure or adhesions in the operated area and this increases morbidity and mortality.4)10) Thus, it was natural that endovascular coil embolization became the alternative treatment modality for remnant or recurred aneurysms. Studies considering endovascular treatment of recurred aneurysms after surgical clipping (Table 2) have reported favorable outcomes and suggest that endovascular coil embolization is a safe and reliable treatment option.2)6)11)12)13) In particular, none of the studies reported procedural-related complications regardless of whether the aneurysm was ruptured or not. Despite these initial promising results, no large-scale study has been conducted, and no long-term follow-up data are available. As some cases are treated for near-complete occlusions, the possibility of recurrence remains. Thus, more reliable studies with a much longer follow-up period and more cases are required.
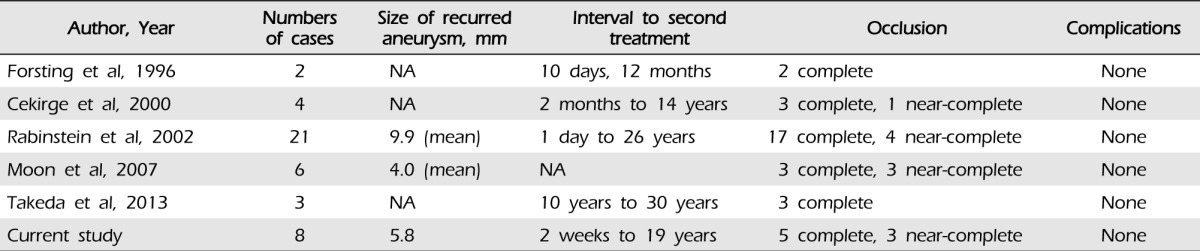
Summary of previously reported studies
CONCLUSION
There are risks of aneurysm recurrence or remnant growth after surgical clipping. In our experience, endovascular coil embolization for the treatment of aneurysm recurrence or remnant was safe and favorable. We observed no procedural-related complications and successful angiographic results were achieved in all cases. Although studies with a longer follow-up period and more cases are required in order to confirm long-term effectiveness, endovascular coil embolization may be a good option for treatment of aneurysm recurrence after surgical clipping.