



INTRODUCTION
The surgical approach of the cavernous sinus (CS) lesion is hard to access. Endovascular treatment of CS lesion is an alternative modality without craniotomy to eliminate the need for additional complication that may arise from microsurgical approach. And the endovascular approach also could reduce the hospital stay with less recovery time. However, complications can still arise from endovascular coil embolization. Thromboembolic events and mass effects are the well-known adverse effects of endovascular treatment. These events are most common during or in the immediate postprocedure period [4]. These complications had been well described, but delayed (>1 year from treatment) nerve palsy after apparently uncomplicated endovascular coil embolization of CS lesion has rarely been reported [2,5]. We describe 2 cases that experienced nerve palsy after coil embolization, and discuss possible mechanisms.
DESCRIPTION OF CASES
Case 1
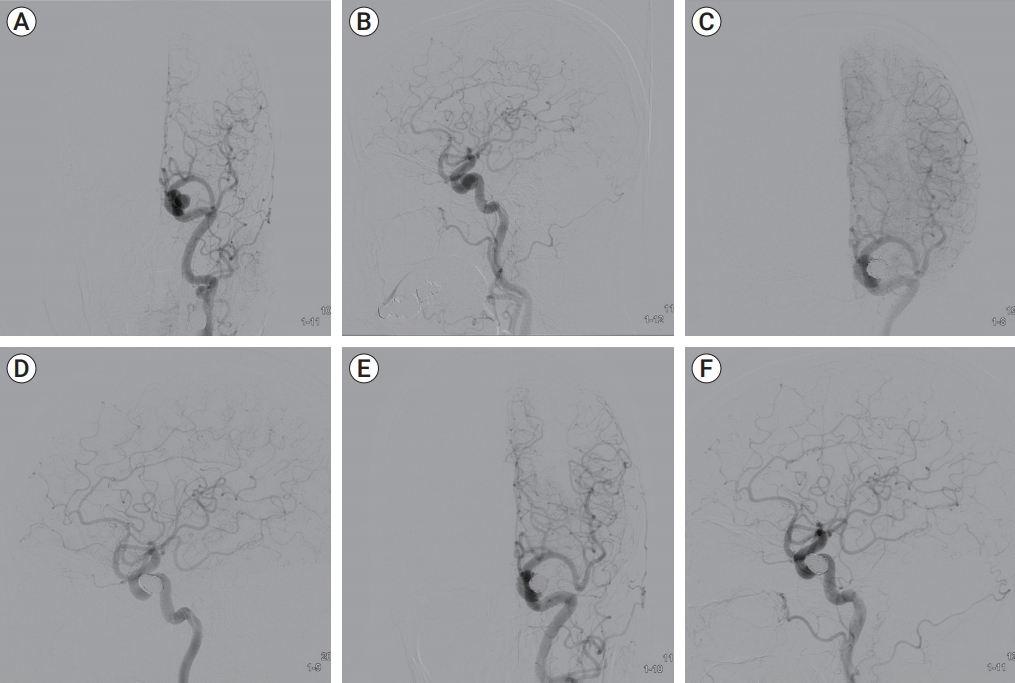
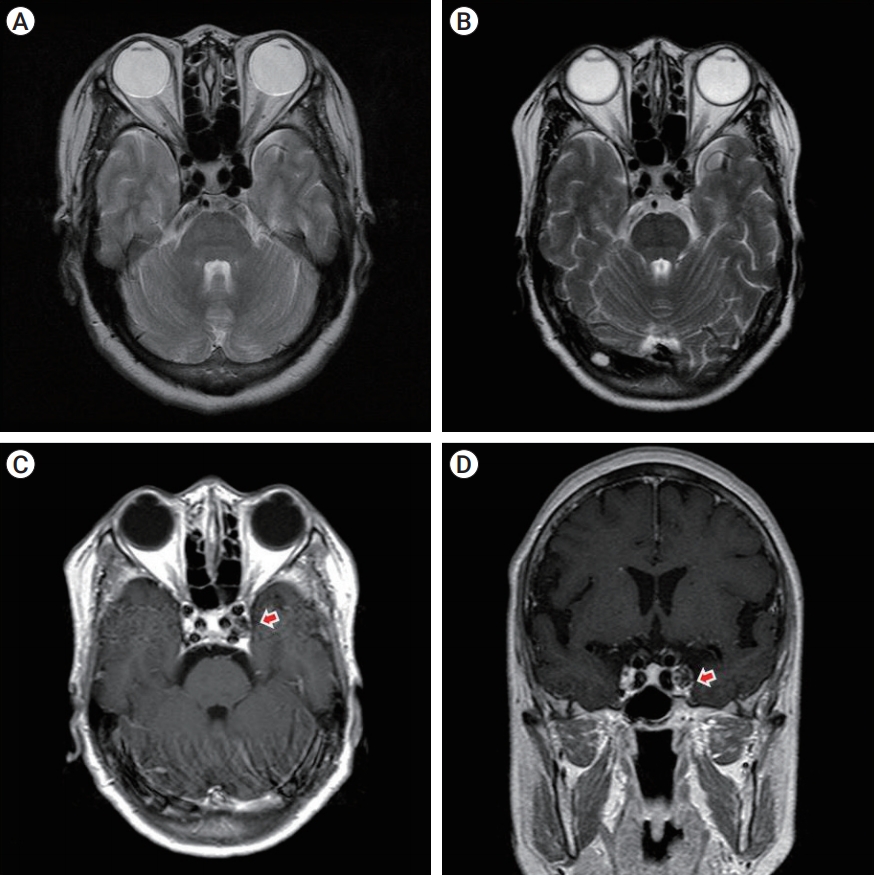
A 61-year-old woman suffered from left hand paresthesia. Angiography demonstrated evidence of incidental unruptured aneurysm (Neck/Height/Width 4.07/12.4/9.2 mm) of the left cavernous internal carotid artery (ICA) (Fig. 1). The aneurysm was embolized with multiple coils (Stryker, Kalamazoo, MI, USA, 360┬░ GDC-18 11├Ś30, GDC-10 SR 10├Ś30, Complex standard 10├Ś30, Complex standard 9├Ś25, GDC-10 2D 9├Ś30, GDC-10 2D 7├Ś25, Complex fill 8├Ś24, total 7) and without any complication, she was discharged (Fig. 1). But 19 months later, she revisited our department due to left side miosis and partial ptosis without anhydrosis (incomplete HornerŌĆÖs syndrome). Laboratory studies and angiography revealed normal findings (Fig. 1). Although magnetic resonance image (MRI) shows no definite enhancement of the aneurysm and CS, T1 weighted enhanced MRI shows discontinuity of left CS outer wall (Fig. 2). We may assume the coils packed in the aneurysm could migrate to the CS through the hole of the aneurysm. The coils sticking out the aneurysmal wall and inflammation could stimulate the sympathetic plexus that surround the ICA. The patient was treated with intravenous corticosteroid. Despite this therapy, the symptoms are continued. Because the patient did not respond to the corticosteroid treatment, we believed that mechanical compression was the more significant contributing factor for the nerve palsy and may have prevented further recovery.
Case 2
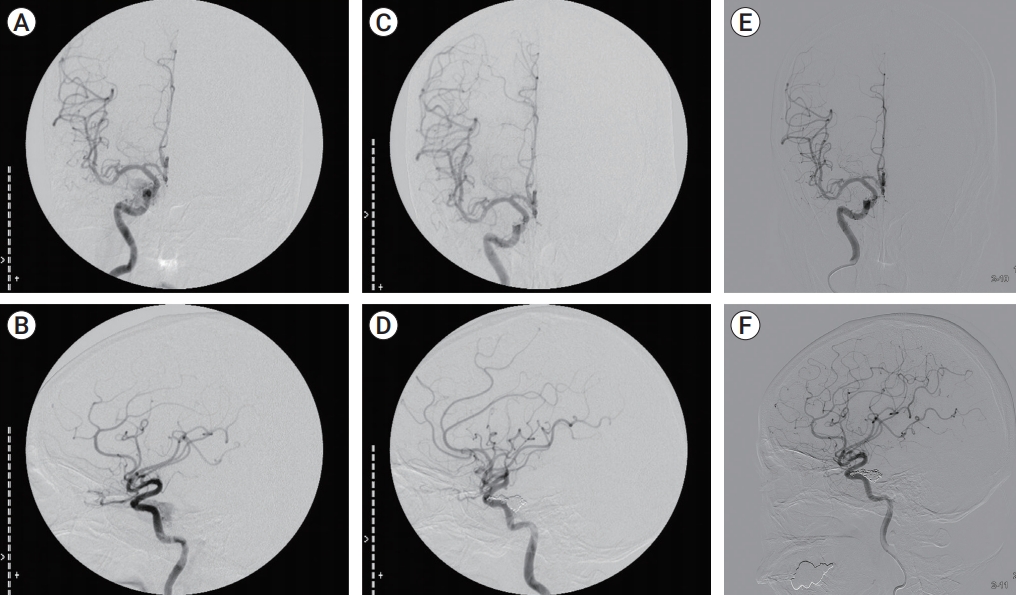
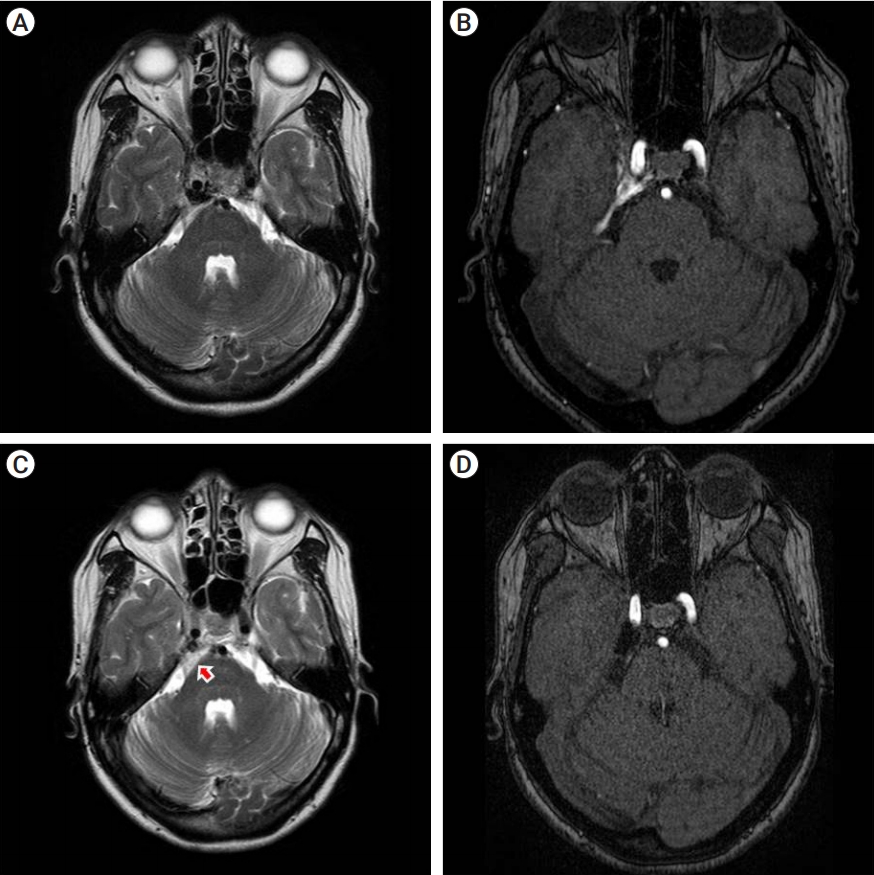
A 50-year-old woman presented right face paresthesia, exophthalmos and ecchymosis for 7 days. Diplopia was not observed and eye movement was in the normal range. MRI and angiography reveal dural type indirect carotid cavernous fistula (CCF). Preoperative T2-weighted axial MRI shows the signal voiding on right CS and preoperative MR source image shows abnormal signal flow on right CS (Fig. 3). Transvenous embolization was taken with multiple coils (Tornado┬« Embolization MicrocoilŌäó, Cook Incorporated, Bloomington, IN, USA, Tornado 5/2├Ś10, Tornado 4/2├Ś9, total 19). She also was discharged without any focal neurologic deficits. After 38 months, she complained of sudden diplopia. The neurological assessment showed restriction in abduction of the right eye (Abducens nerve impairment). Laboratory tests showed normal limits. Postoperative T2-weighted axial MRI shows some mixed signal intensity lesion around CS and prepontine/superior cerebellopontine cistern, suggesting inflammatory reaction or thrombosis (Fig. 4, C, arrow). But no abnormalities were observed in the hematological examination of the patients. And postoperative MR source image reveals complete obliteration of CCF. After steroid pulse therapy, the diplopia much improved. This cranial nerve palsy may be stabilized with the administration of corticosteroid. Although we could not check follow up MRI, we think the cause of this cranial nerve palsy is inflammatory reaction around the CS.
DISCUSSION
CS lesion is hard to access by surgical approach. With advance of endovascular technique and device development (microcatheter, microwire and embolization materials), it is becoming the main treatment modality of the CS lesions [3]. Endovascular treatment of CS lesion is an alternative modality without conventional craniotomy and according complications. And it also could reduce hospital stay and recovery time.
Although it has many advantages, complications can still arise from endovascular coil embolization. Categorization of complications after endovascular treatment can be based on the mechanism, etiology and symptom onset timing [10]. The most common and serious neurological complication is thromboembolic stroke, which occurs abruptly and is maximal at onset [4,10]. These events are most common during the procedure or in the immediate postprocedure [4]. These ischemic deficits typically do not improve with time or respond to corticosteroid therapy and may require emergent intervention to reperfusion of the occlude vessels and to recover the nerve injury [10]. Kim et al. report newly developed cranial nerve palsy after transvenous coil embolization. The reason for cranial nerve palsy may be due to progressive thrombosis of the CS, the mass effect due to the packed coils and direct injury by the coil or microwire/microcatheter [6,7]. Progressive cranial nerve palsy typically occurs hours to weeks after the endovascular procedure. Unlike the thromboembolic events, progressive cranial nerve palsy has a slower and more progressive onset. It is likely secondary to evolving mass effect from aneurysm thrombosis with/without perianeurysmal inflammation and edema, or from aneurysmal growth, or from a combination of both processes [8-10]. These nerve palsy may be stabilized or improved with the administration of corticosteroid. These complications described on the above paragraph; occur within a few weeks after coil embolization.
In our cases, however, nerve palsies occurred after 1 year from successful embolization. Delayed (>1 year from treatment) nerve palsy after endovascular coil embolization of CS lesion was rare [2,5]. In generally, after obliteration of the aneurysm by coil embolization, the aneurysmal wall became disorganized from invasion by capillaries and fibroblasts, organization of the thrombotic material, and the initiation of a chronic foreign body reaction in the neighborhood of the coils [1]. The chronic inflammation may cause thickening of the aneurysm wall, making this thicken wall is an important protective mechanism to prevent aneurysm rupture [9]. But in case 1, we hypothesis the coils packed in aneurysm could migrate to the CS through the hole of the aneurysm. The coils sticking out the aneurysmal wall and some inflammation could stimuli the sympathetic trunk that surrounding the ICA. In case 2, we could not explain the inflammation occurred too late after coiling. MRI reveals at this stage of inflammation but could not prove the cause of this inflammation. We doubt that probable recurrence of CCF that was not seen in MRI. So repeated angiogram was recommended, but she declined further intervention. We thought about the location of coils because coil packing in the posterior cavernous sinus can induce the abducent nerve palsy, but it didnŌĆÖt explain the reason why the delayed the abducent nerve palsy occurred.
CONCLUSIONS
We report 2 cases of delayed cranial nerve palsy after successful coil embolization. The cause is still undefined. We should keep in mind that the delayed cranial nerve palsy could be happen after successful coil embolization of cavernous ICA aneurysm or CCF and in these cases, additional treatment such as steroid treatment can be used.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






