A Protocol-Based Decision for Choosing a Proper Surgical Treatment Option for Carotid Artery Stenosis
Article information
Abstract
Objective
There are two established surgical treatment options for carotid artery stenosis. Carotid endarterectomy (CEA) has been accepted as a gold standard for surgical treatment while carotid artery stenting (CAS) has recently become an alternative option. Each treatment option has advantages and disadvantages for the treatment outcomes. We propose a protocol for selection of a proper surgical treatment option for carotid artery stenosis.
Materials and Methods
A total of 192 published articles on management of carotid artery stenosis were reviewed. Preoperatively considerable factors which had been repeatedly noted in those articles for the risk/benefits of CEA or CAS were selected. According to those factors, a protocol with four categories was established.
Results
CEA or CAS is indicated when the patient has a symptomatic stenosis ≥ 50%, or when the patient has an asymptomatic stenosis ≥ 80%. Each treatment option has absolute indications and favorable indications. Each absolute indication is scored with three points, and each favorable indication, one point. Based on the highest scores, a proper treatment option (CEA or CAS) is selected.
Conclusion
We have been treating patients according to this protocol and evaluating the outcomes of our protocol-based decision because this protocol might be helpful in assessment of risk/benefit for selection of a proper surgical treatment option in patients with carotid artery stenosis.
INTRODUCTION
Currently, there are two surgical treatment options for carotid artery stenosis, carotid endarterectomy (CEA) and carotid artery stenting (CAS). CEA has long been established as the gold standard for treatment of severe symptomatic carotid artery stenosis.6)9)18)23)29)32) As CAS has become an alternative treatment option, it is difficult to decide which treatment option, CEA or CAS, is appropriate for patients with carotid artery stenosis.5) Each procedure has its own risks.2)5)23)25)35)44) In addition, various factors, such as patients' factors or radiographic data, could be related to the risk for these preventive procedures and should be categorized as favorable or unfavorable to each procedure. Also, it is important to recognize and understand limitations of published evidence regarding which surgical treatment option is better than the other.
Yet, no guidelines have been established for deciding on a proper surgical treatment option between CEA and CAS according to the benefits and risks of each procedure in institutions where both CEA and CAS are available. Thus, we propose a protocol for selection of a proper surgical treatment option for carotid artery stenosis.
MATERIALS AND METHODS
Eligibility for surgical treatment
A multidisciplinary team including neurosurgeons, neurologists, and radiologists participated in development of a protocol for selection of a proper surgical treatment option. Indications for surgical treatment (CEA or CAS) of patients with carotid artery stenosis were decided according to three international guidelines, the European Union Stroke Initiative clinical guidelines, the North American Symptomatic Carotid Endarterectomy Trial criteria, and the American Stroke association, with high level of evidence.4)10)25)30)32) Patients satisfying the indications were considered for the treatment.
Search strategy and making a protocol
A search for systematic literature review was performed using the key words "Carotid artery stenosis" or "Carotid endarterectomy" or "Carotid artery stenting" or "Carotid stenting versus endarterectomy" on PubMed and Medline. A total of 192 published articles written in English were selected and were reviewed independently by three authors. Among the 192 articles, 28 articles were selected as references for this study and they all met following criteria: 1) single or multiple randomized clinical trials, 2) review articles in journals with high impact factors (≥ 6), or 3) well-designed case-control studies including a large number of patients.
From those articles, we selected preoperatively considerable factors which had been repeatedly noted in several chosen articles for risk/benefits of CEA or CAS.7)9)18)19)23)29)31)32)35)38)50) According to those factors, we made a general outline of our protocol. Then, we descended to particulars in order to specify exact indicative values for each factor suitable for our institution.
Preoperative evaluation
Preoperatively, clinical evaluation was performed for the neurological assessment including the National Institutes of Health Stroke Scale.28) Radiographic evaluation was also performed, such as carotid artery computed tomography (CT), magnetic resonance angiography (MRA), and digital subtraction cerebral angiography (DSA). Routine echocardiogram was also performed for evaluation of cardiac function and possible sources of embolus.
RESULTS
This protocol was designed for mainly elective cases and was focused on the patient with a symptomatic carotid artery stenosis ≥ 50%, an asymptomatic stenosis ≥ 80%, or an asymptomatic stenosis ≥ 50% with contralateral carotid artery occlusion. Emergent cases, such as acute ischemic stroke due to or combined with carotid artery stenosis, as well as strong preference of patients for a certain treatment option were considered as an exceptional situation.
We have established a protocol with four categories based on the selected factors, which were difficulties of anatomic approach to the carotid artery either by CEA or CAS, cardiopulmonary function (evaluated by echocardiogram and pulmonary function test), existence of renal failure, a previous history of neck treatment (neck surgery or radiation), contralateral laryngeal paralysis, allergic reaction to contrast medium, vascular access for diagnostic DSA, calcification around the carotid artery stenosis (evaluated by carotid artery CT), complicated atheroma on the ascending aortic arch (evaluated by echocardiogram), string sign, ulcerated stenosis (evaluated by DSA when it was seen as a crater from the lumen into a stenotic plaque), the length of the lesion, and the existence of tandem stenosis (multifocal stenosis from the proximal cervical to the distal internal carotid artery or to the ipsilateral middle cerebral artery), contralateral carotid artery occlusion, and poor collateral flow of the anterior communicating artery.5)6)11)12)14)15)16)17)20)22)23)24)26)27)31)33)34)40)41)42)43)46)48)49)
Table 1 shows our protocol for selection of a proper surgical treatment option for carotid artery stenosis. Each treatment option (CEA or CAS) had absolute and favorable indications. A simple numerical score was assigned for those indications. We granted the weight to the absolute indications three times rather than the favorable indications because the absolute indications have been debated in several articles including major randomized controlled trials and were considered as "absolute." Thus, we discussed and decided that one absolute indication should be considered more important than two favorable indications. Therefore, each absolute indication was scored with three points, and each favorable indication, one point. Based on the highest scores, a proper treatment option (CEA or CAS) can be selected. If the score was the same, patient preference would be a key to selection of a treatment option.
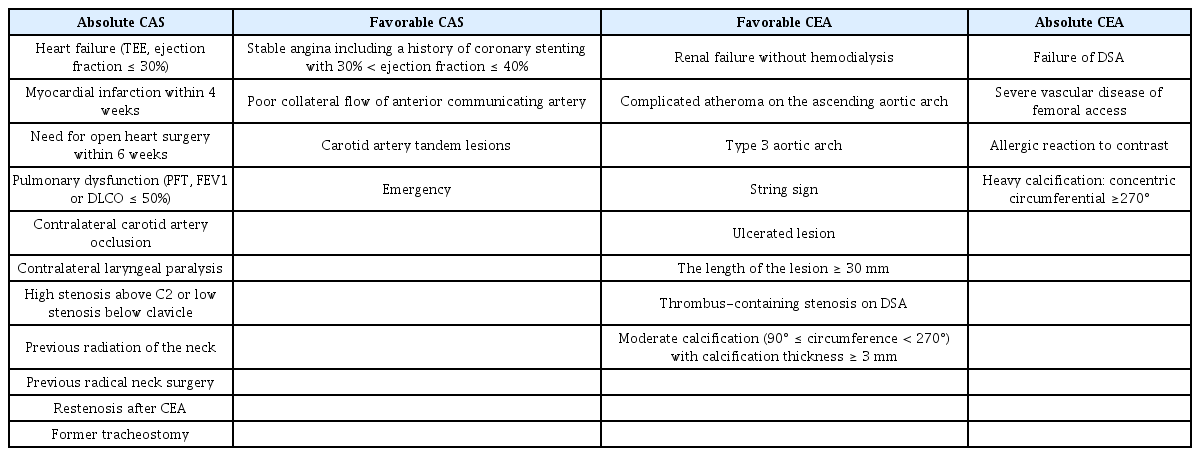
Protocol for selection of a proper surgical treatment option for carotid artery stenosis
Absolute indications for CEA
CEA is chosen over CAS in cases of failed DSA,12) severe vascular disease of femoral access,27) allergic reaction to contrast,26) or heavy calcification around the carotid stenosis with a concentric circumference ≥ 270 degrees.12)20)26)27)38)40)
Favorable indications for CEA
CEA may be chosen over CAS in cases of renal failure without hemodialysis,34)46) complicated atheroma on the ascending aortic arch,11)23) type 3 aortic arch, the string sign,21)24) thrombus-containing lesion on DSA,21)23) presence of ulcerated lesions,16)22) the length of the lesion ≥ 30 mm,14)17)42)49) or moderate calcification around the carotid stenosis with a circumference between 90 and 270 degrees with maximal thickness of calcified plaque ≥ 3 mm.20)39)41)
Absolute indications for CAS
CAS is chosen over CEA in cases of heart failure (ejection fracture ≤ 30%),5)31)41)44) myocardial infarction within 4 weeks,5)31)33) need for open heart surgery within 6 weeks,5)31)40) pulmonary dysfunction (forced expiratory volume in 1 second or diffusion capacity for carbon monoxide ≤ 50%),31) contralateral carotid artery occlusion, contralateral laryngeal paralysis, high stenosis above the C2 body, low stenosis below the clavicle, previous radiation of the neck, previous radical neck surgery, restenosis after CEA, or former tracheostomy.6)48)
Favorable indications for CAS
CAS may be chosen over CEA in cases of stable angina including a history of coronary stenting with ejection fraction between 30% and 40%,5)31)40)44) poor collateral flow of the anterior communicating artery,40) carotid artery tandem lesions,49) or in emergent cases, such as thrombolysis or thrombectomy in patients with acute ischemic stroke due to or combined with carotid artery stenosis.
DISCUSSION
By reviewing recent evidence, we understood that the risk of periprocedural stroke was lower for CEA than CAS in symptomatic patients and octogenarians. In addition, more data from long-term follow-up was available for CEA than CAS. However, CEA showed higher risk of periprocedural myocardial infarction, cranial nerve damage, and wound complications than CAS. Also, in most cases CEA required general anesthesia and a longer recovery period than CAS.
After understanding those concepts from recent evidence, we proposed a protocol for selection of a proper surgical treatment option for carotid artery stenosis according to various factors which had been noted in several articles including the major randomized controlled trials. If the procedure of CEA or CAS became complicated, procedure-related complications could increase and clinical outcomes would be poor. Thus, we would like to develop a scoring system for assessment of risk/benefit of CEA or CAS. And, we expected that this protocol might be helpful for assessment of risk/benefit for selection of a proper surgical treatment option in the future. We have been evaluating the outcomes and complications of our protocol- based decision.
This protocol was designed for mainly elective cases and we usually performed CEA or CAS within 14 days of acute stroke events in patients with symptomatic lesions.9) Previously, early treatment within two weeks of acute stroke could increase the risk of the treatment.3) However, recent analysis showed that delayed surgery after 2 weeks of acute stroke events did not reduce the risk of the treatment but increased the risk of recurrent events of stroke.38) In addition, the surgical treatment was safe and most effective when performed within 2 weeks of the patient's last symptoms.1)8)36)37) Patient's age was not included in this protocol. Stroke guidelines recommended that it is reasonable to consider patient age in choosing between CAS and CEA. For older patients (octogenarians), CEA may be associated with improved outcome compared with CAS, particularly when arterial anatomy is unfavorable for endovascular intervention.9) In addition, the Carotid Revascularization Endarterectomy versus Stenting Trial (CREST) investigators showed that younger patients had relatively lower risk of stroke and older patients had higher relative stroke risk in the CAS group than in the CEA group.45) However, after discussing patient age, we decided to ignore patient age and to consider individual physical capability. We thought that age itself did not affect the risk/benefit of CEA or CAS, but age-related comorbidities, such as cardiopulmonary problems, unfavorable vascular anatomy, or characteristics of stenosis, did affect the risk/benefit. Thus, we included those comorbidities in our protocol rather than patient age.
In our institution, CEA has been performed under general anesthesia. Because cardiopulmonary dysfunction is a possible risk factor of general anesthesia, it can work against CEA. In addition, death due to cardiac origin is a well-known disadvantage of CEA. Thus, we included cardiopulmonary dysfunction as an indication for CAS. Patients with a history of coronary artery disease had a 6.5-fold increased rate of postoperative non Q-wave myocardial infarction.31) Also, there is a 3-fold higher risk of ipsilateral stroke in patients with myocardial infarction, congestive heart failure, atrial fibrillation, left ventricular hypertrophy, and oxygen dependent pulmonary disease compared to those without such medical risk factors.31)33)40) Patients with stable angina including a history of coronary stenting with ejection fraction between 30% and 40% were at risk of postoperative ischemic attack.31)
We preferred CEA for calcified stenosis because calcification around the carotid artery stenosis was an important predictor of complications of CAS in several studies.20)39)41) Heavy calcification in combination with arterial tortuosity caused difficulties in stent positioning, lesion dilatation, and adequate stent expansion.39) This might be related to new post-procedural ischemic injuries.20)39)41) Thus, we included calcification around the stenosis as an indication for CEA.
Potential embolic sources during the procedure of CAS, such as atherosclerotic aortic lesions, the string sign, or the presence of ulcerated lesions, were categorized to favorable indications for CEA. These factors could be associated with thromboembolic events with a high incidence of ischemic complications during CAS and make CAS complicated.7)11)13)16)18)21)22)24) In addition, the length of the lesion ≥ 30 mm required the use of longer stents of multiple stents,17)49) which could increase the technical complexity of CAS and result in poor clinical outcomes. Patients with renal failure without hemodialysis were considered for CEA because nephrotoxicity induced by contrast medium was associated with the potential need for renal replacement therapy and increased mortality.47) If patients with end stage renal disease underwent dialysis, CAS could be performed without concern for contrast-induced nephropathy.
CONCLUSION
We have been treating the patients according to this protocol and evaluating the outcomes of our protocol-based decision because this protocol might be helpful in assessment of risk/benefit for selection of a proper surgical treatment option in patients with carotid artery stenosis. Our results with short- and long-term follow-ups will be reported.
Notes
Disclosure: The authors report no conflict of interest concerning materials or methods used in this study.
