


INTRODUCTION
Endovascular procedures are increasingly being used to treat various cerebrovascular disease entities like aneurysm, arteriovenous malformation, tumor embolization, stroke thrombolysis and thrombectomy, middle meningeal artery embolization for chronic subdural haemorrhage, carotid stenosis, cerebral venous thrombosis, dural fistulas, etc. Trans-femoral is considered as classical approach over trans-radial, and hence is increasingly being performed in contemporary times, allowing for unlimited repetition of puncturing, easy access, less radiation time and less contrast usage [1]. Complications include hematoma, bleeding, pseudoaneurysms, fistulas, retroperitoneal haemorrhage, venous puncture, dissection, etc. and they have been well reported, when the puncture is inappropriate [5]. However, among rarely reported complications due to hardware failure owing to intraluminal knotting, unravelling, most of them have been for central venous cannulation, specifically for subclavian vein, most likely due to curved path of the vein over first rib [3,4]. Such complications while cannulating and decannulating the femoral artery are scarcely reported.
ILLUSTRATIVE CASE
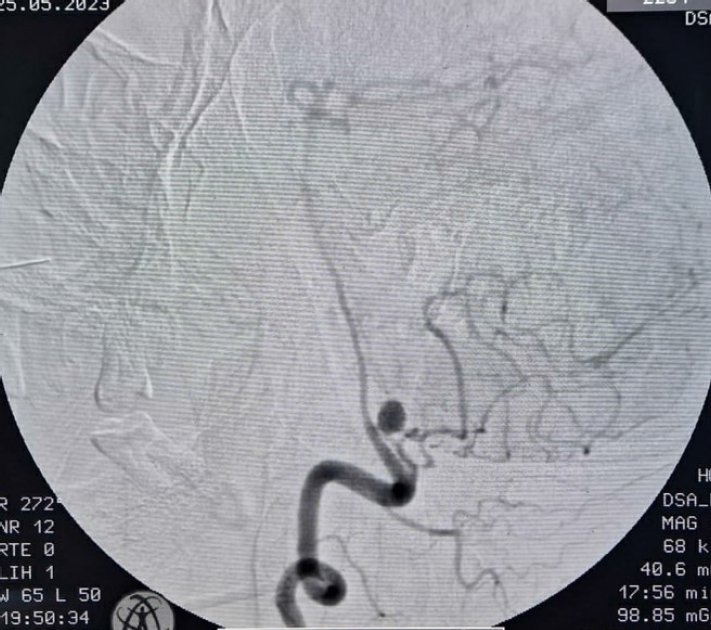
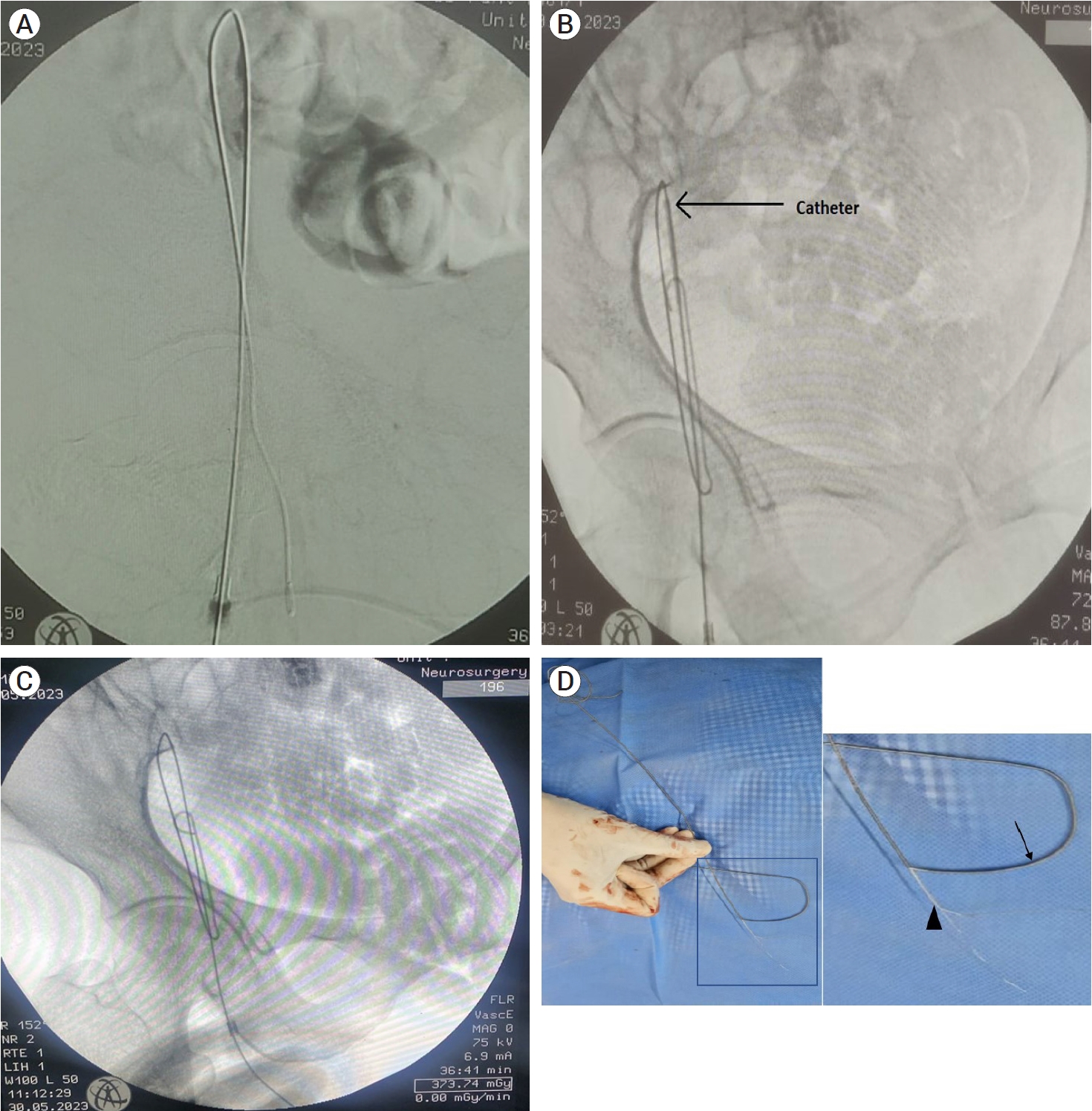
A 55 year old, moderately built female, on presenting with headache, was diagnosed with unruptured right proximal posterior inferior cerebellar artery (PICA) aneurysm (Fig. 1) by diagnostic cerebral digital substraction angiography (DSA), which was uneventfully accomplished by right femoral artery access in first attempt with smooth cannulation via single wall Seldinger technique. Subsequently, after 2 days, she was taken up for therapeutic intervention by endovascular coiling, for which again percutaneous right femoral access was planned by manual palpatory method, via entry point 1.5 cm below the mid inguinal point. After initial puncture with single wall Seldinger technique using 18G puncture needle, guide wire (diameter 0.038ŌĆØ, length 45 cm, J tip) was introduced, which went through with little resistance. Puncture needle was removed, and 7F introducer sheath was threaded over the wire as standard practice, after placing the nick on skin and subcutaneous tissue. On attempting to withdraw the wire with introducer sheath, significant resistance was encountered, resulting in failure of removal. Immediately, puncture site was visualised under fluoroscopy guidance, and guide wire was found to be bent, with an inferiorly directed loop in the femoral artery (Fig. 2A). However, position of introducer sheath was confirmed in the lumen by good back flow of blood from the side channel. Multiple attempts were made to remove the wire by to and fro movement, by pushing it to straighten it, by pulling it against resistance, but everything failed. Instead of straightening, the wire looped several times (Fig. 2B). Next, an attempt was made to pass a 5 French multipurpose catheter (MPC) over the wire through the diaphragm of the check flow, which could only be negotiated till the first bend of wire (Fig. 2C). The discrepancy in the length of MPC (90 cm), over the wire (45 cm), was resolved by cutting the MPC, till proximal part of guide wire was visualised. Introducer sheath was withdrawn, and attempt was made to remove the entire assembly en masse, which also failed. Cardiothoracic and Vascular surgeonsŌĆÖ team was summoned for help and planned for arteriotomy and removal, during which, after removal of MPC, it was noticed that distal guide wire was broken and had gotten separated into rigid straight central core and overlying soft coiled part which became unravelled (Fig. 2D). On final attempt by grasping the rigid core wire, using improvised rotational manoeuvre simultaneously with pulling, the proximal end got dislodged and retrieval was successful. Immediately the access site was compressed manually, after haemostasis was ensured, good femoral and dorsalis pedis pulsations were palpable. The coiling of aneurysm was then completed successfully via left femoral artery puncture and patient was discharged uneventfully.
DISCUSSION
Intravascular knot formation, unravelling, knotting and kinking of guide wire is common for central venous cannulations, literature regarding knot formation while cannulating the artery in one attempt is scarce, and retrieval of such kinked and unravelled wire, without major morbid complications is even scarcer [2]. Here, the suspected causes are speculated to be overly malleable and faulty guide wire, inadequate nick over skin and subcutaneous tissue leading to introducer sheath tip damage due to forceful insertion against resistance (damaged tip can damage the wire as well as intima during manipulation), repeated attempt via the same side within short interval, and forceful introduction of wire against even slight resistance. One must exert extreme caution while selecting the entry point, and inspect the hardware minutely before the procedure, and keep extremely low threshold for resistance and manoeuvring difficulties, to avoid such incidents.
CONCLUSIONS
Complications like these are extremely uncommon and their unpredictability makes them difficult to manage. Before attempting forceful introduction or removal of guide wire, the target site should be visualised under fluoroscopic guidance to confirm the point of resistance and status of guide wire in the lumen.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






