



INTRODUCTION
Arteriovenous malformations (AVMs) are abnormal collections of feeding arteries and draining veins connected in the absence of an intervening capillary bed, which leads to arteriovenous shunting of blood through a central nidus. While AVMs may occur in any region of the brain, it is exceedingly rare for them to involve the choroid plexus of the ventricular system [4,5,9]. Roughly 5-15% of all intracranial AVMs are located within the ventricles of the brain with only a small minority of those involving the choroid plexus [1,14]. Given the rarity of this condition, the current literature describing choroid plexus AVMs consists almost entirely of case series and individual case reports. As a result, there is limited consensus on the safest and most efficacious treatment for choroid plexus AVMs, which makes decision-making challenging. The purpose of this study was to systematically review the reported outcomes and complications of different treatment options for choroid plexus AVMs, specifically focusing on surgical resection and endovascular embolization.
METHODS
Literature search
A systematic literature review was performed on PubMed using search terms such as ŌĆ£choroid plexus arteriovenous malformation,ŌĆØ ŌĆ£choroid plexus AVM,ŌĆØ ŌĆ£ependymal AVM,ŌĆØ and ŌĆ£ventricular AVMŌĆØ. Selection criteria included studies published between January 1975 and July 2021 describing the clinical presentation, management, and/or outcomes of confirmed cases of AVMs in the choroid plexus. Additional articles cited in the studies that resulted from the initial PubMed search that also met inclusion criteria were included in the final analysis. Both adult and pediatric patients were included for analysis.
Literature review and data extraction
No registered review protocol was used in this systematic review. This study follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Patient demographics, diagnostic method, treatment modality, clinical outcomes, and complications were recorded. Approval from the institutional review board and patient consent were not necessary due to the use of publicly accessible data for this study. Early morbidity was defined as morbidity in the immediate postoperative period. Classification of improved, stable, and worsened neurologic function was based on the definition used in each study, which was most commonly based on clinical evaluation.
Statistical analysis
Descriptive statistics for continuous variables are reported as mean and standard deviation while that for categorical variables are reported as number of patients and percentage. All statistical analyses were performed using Stata [19].
RESULTS
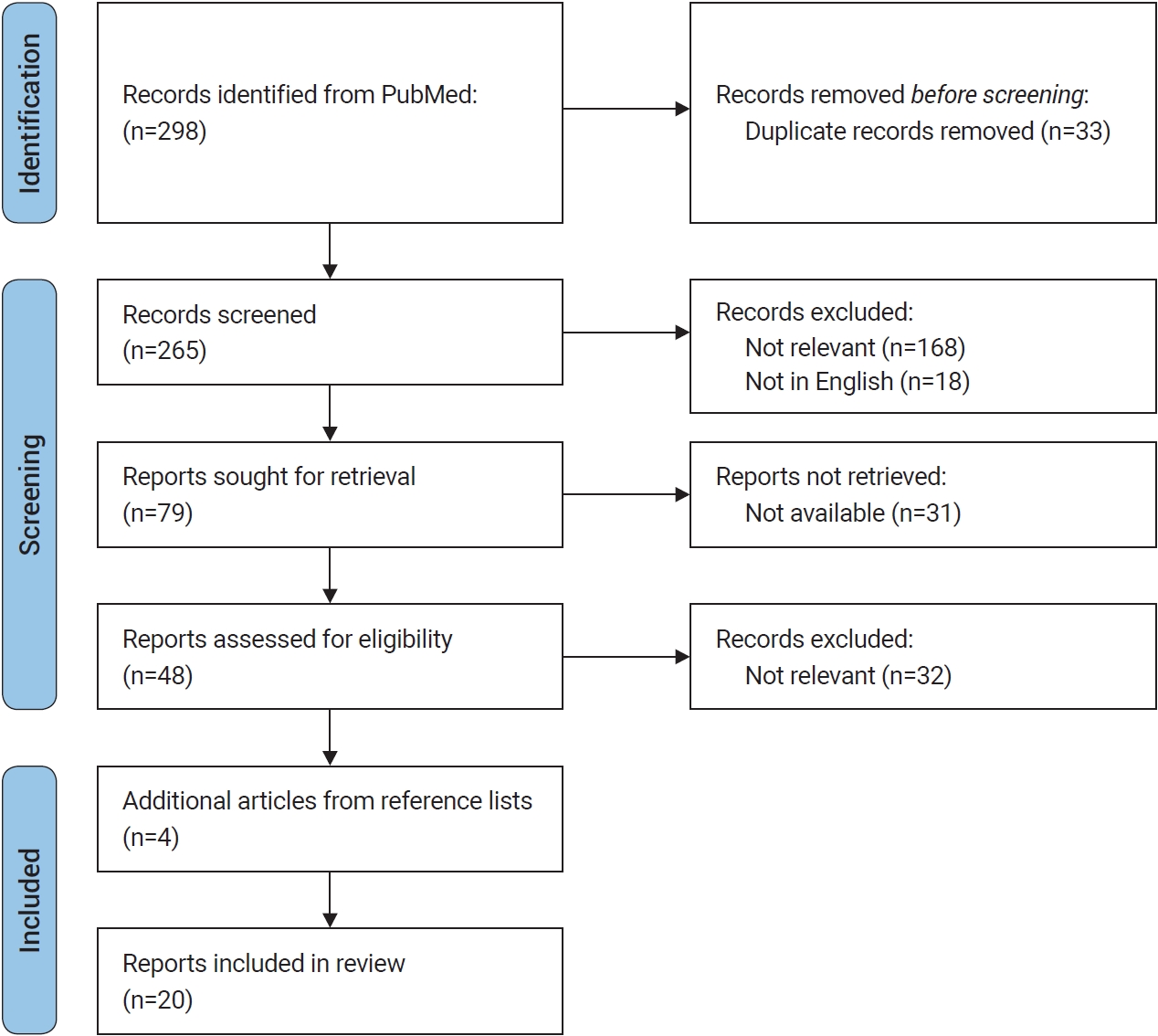
The literature search yielded 298 articles published between January 1975 and July 2021. Of those, 55 articles were duplicate records and subsequently removed. Upon initial screening of the remaining 265 articles, 186 were excluded: 168 were not relevant while 18 were not in English. Additionally, 31 articles were not available for retrieval. A total of 48 articles were thus reviewed and assessed for eligibility. During this round of screening, 32 reports were excluded based on relevance whereas 4 articles identified from the reference lists were added. A total of 20 studies were included in the final analysis. Of these, 18 were single-patient case reports [1-4,6-13,15-17,20-24], one article contained 2 patients [21], and a single study was a cohort of 24 patients [15]. Fig. 1 summarizes the systematic review process.
All single patient studies, as well as each of the patients of the two-patient study are presented in detail in Table 1, for a total of 20 patients. Patient age ranged from one day to 61 years, with a mean of 31.8┬▒20.4 years. Ten patients were female (50.0%) and 10 were male (50.0%). Most choroid plexus AVMs were located in the lateral ventricles (14 patients, 70.0%), while there were 4 (20.0%) located in the third ventricle, and two in the fourth ventricle (10.0%). Among the 14 lateral ventricle AVMs, seven (50.0%) were left-sided, six (42.9%) right-sided, and for one (7.0%), laterality was not reported. Four reports included size measurements, specifically, a 61-year-old male with an AVM 2 cm in diameter, and a 12-year-old male with a 1.5 cm AVM. A 55-year-old female was reported to have an 8-cc lesion in volume, and a 1-day-old male had a 1 cc lesion in volume. The rest of the reports did not mention either diameter or volume. Arterial feeders included the anterior choroidal artery in six patients (50.0%), the posterior lateral choroidal arteries in nine (75.0%), the cavernous ICA in one patient (8.3%), and the middle meningeal artery in one patient (8.3%). Arterial supply was not specifically mentioned or was unable to be ascertained in six cases. Venous drainage was deep in all mentioned cases. The internal cerebral veins were the primary drainage site in five patients (62.5%), the vein of Galen in two (25.0%), and the basal vein of Rosenthal in one case (12.5%). Venous drainage was unable to be ascertained or was not mentioned for 12 patients. A total of 13 patients (65.0%) had a hemorrhagic presentation, either an intraventricular, subarachnoid, or intraparenchymal hemorrhage. AVM diagnosis was based on digitally subtracted angiography (DSA) for 13 patients (65.0%), while five (25.0%) were diagnosed based on final pathology. Diagnosis was based on computed tomography (CT) scan for one patient (5.0%) and magnetic resonance imaging (MRI) for one patient (5.0%).
Almost all patients were treated by surgical resection (18 patients, 90%). In 14 of these patients (77.8%), complete resection of the AVM was achieved. A residual AVM was reported in a single case (5.6%). Three cases (16.7%) did not report whether a residual lesion remained following resection. The remaining two patients (10.0%) were treated by endovascular embolization rather than surgical resection. Both cases reported residual AVM after embolization. Most patients were reported to improve from their presentation status over time (14 patients, 70.0%). A single patient was reported to have died 22 hours after admission due to massive intracerebral hemorrhage due to ruptured AVM. One patient was reported to be ŌĆ£stableŌĆØ after his resection with no improvement or worsening, and one patient was reported to have a cerebral infarction of the left optic radiation resulting in e.g.right homonymous hemianopsia, a worsening of his state at presentation. For three patients (15.0%), long-term outcome was not reported. The follow-up period was reported for seven patients with a mean of 7.7┬▒4.1 months. Presence or absence of long-term sequelae (e.g., neurologic deficits) were reported for 14 patients (70%). Eleven of these patients (78.6%) were reported to have no neurological sequelae, one patient had long-term gait instability, one patient had right-sided homonymous hemianopsia, and one patient was reported to have developed hydrocephalus, requiring shunting.
A single study by Miyasaka et al. [15] reported 24 choroid plexus AVMs, the largest case series to date. The series included 10 females (41.7%) and 14 males (58.3%), with an age range of eight to 47 years (mean 27). Of the 24 patients, 22 presented with intracranial hemorrhage (91.7%) and two with seizures (8.3%). All lesions involved the lateral ventricles, and side was not specified. All lesions were diagnosed with DSA, were resected, and were histologically verified. Outcomes were assessed based on the Glasgow Outcome Scale (GOS). A total of 19 patients (79.0%) were reported to have ŌĆ£good recoveryŌĆØ. Three patients (12.5%) had moderate disability, and two patients (8.3%) died due to postoperative hemorrhage of residual AVM nidus.
DISCUSSION
AVMs are abnormal collections of arteries and veins connected in the absence of an intervening capillary bed. They are believed to arise during fetal development when fistulas develop at crossings between arterial and venous endothelial tubes or when primitive channels fail to be resorbed [18]. Intracranial AVMs are detected at a rate of about 1 to 2 per 100,000 person-years; however, AVMs limited to the choroid plexus of the ventricular system are exceedingly rare [5]. Between January 1975 and July 2021, only 20 articles comprising 44 patients were identified with the majority of cases described as individual case reports. While reports in the current literature are scarce, the true incidence of choroid plexus AVMs is unknown given that many are clinically silent and may go undetected even at autopsy unless the choroid plexus is intentionally and systematically examined [2,18].
Choroid plexus AVMs may differ significantly in size and location, however, they are thought to occur most commonly in the lateral ventricle, which is consistent with the findings of this review [9,21]. The natural history and clinical presentation of AVMs within the choroid plexus can also vary considerably, ranging from asymptomatic and undetected to sudden non-traumatic death. They are often asymptomatic at birth, thus going undiagnosed unless they rupture or cause other neurologic symptoms [4,5]. The most frequent presentation among all AVMs is intraventricular hemorrhage with the tendency for bleeding higher in children (80%) compared with adults (50-65%) [1]. The results of this study suggest that the majority (65%) of symptomatic patients have a hemorrhagic presentation with either an intraventricular, subarachnoid, or intraparenchymal hemorrhage. Prognosis is also thought to be correlated with the severity of intracerebral bleeding [17]. Other common clinical manifestations that lead to discovery of these lesions include seizures, hydrocephalus, progressive neurological deficits, and sudden-onset headache, nausea, and vomiting [14].
The majority of known choroid plexus AVMs have been treated with surgical resection (90%), while only two patients have been treated with angiographic embolization (10%). Previously, choroid plexus AVMs have been reported to be associated with a higher rate of residual niduses (nearly 30%) compared to AVMs in other locations (roughly 10%) [15]. A residual AVM was shown in only one patient treated with surgical resection (6.7%) whereas both patients treated with angiographic embolization were left with residual niduses (100%). These results suggest that surgical resection has a high success rate when it comes to removing the entire malformation. In contrast, embolization is measured based on complete or partial occlusion of the AVM nidus rather than complete removal. Clinically, 70% of patients who underwent treatment for choroid plexus AVM (surgical or angiographic) improved symptomatically. In addition, of the patients who were followed for long-term sequelae, almost 80% had no neurological sequelae. This demonstrates not only that choroid plexus AVMs are treatable, but that their treatment does not necessarily lead to adverse effects in the majority of individuals. In addition, even after an acute hemorrhage, resection has been shown to result in ŌĆ£good recoveryŌĆØ in almost 80% of patients. This implies that surgical resection is not only a relatively safe procedure, but it can also be used in acute settings with a good success rate when it comes to immediate recovery and long-term neurological sequelae.
Limitations
This review is limited by the retrospective, singlecenter case reports and case series that comprised the pooled data. As such, publication bias represents a major limitation of this review given the collection of single case reports in this analysis. Cases of choroid plexus AVMs with poor clinical outcomes may not have reached publication, which would result in a literature review that preferentially identifies studies that report successful treatment. The articles included were also published for a variety of purposes, from discussing surgical approaches for resection to classifying types of choroid plexus AVMs. Additionally, there were differences in outcome reporting scales, severity of symptoms, and length of follow-up among the included cases, which reduced the uniformity and generalizability of the data. Furthermore, the data used in this analysis are from different epochs spanning between 1975 and 2021, during which there were significant changes in imaging technology, surgical techniques, and available interventions, which makes it difficult to compare results across these time periods. Nonetheless, these data represent a summary and analysis of the available data on the management and outcomes of this rare disease entity.
CONCLUSIONS
While data on choroid plexus AVMs remains limited, the available evidence suggests gross total resection of lesions in this location can be safely achieved with subsequent reduction in preoperative symptoms. Additional studies are needed to further characterize methods of choroid plexus removal, their risks, and long-term sequelae.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






