Communicating Hydrocephalus Accompanied by Arachnoid Cyst in Aneurismal Subarachnoid Hemorrhage
Article information
Abstract
The authors describe a case of communicating hydrocephalus accompanied by an arachnoid cyst in an aneurismal subarachnoid hemorrhage. A 69-year-old female was referred to our clinic due to the sudden onset of a headache. A head computed tomography scan demonstrated an arachnoid cyst in the right middle fossa with a mass effect and diffuse subarachnoid hemorrhage. Digital subtraction angiography then revealed a left internal carotid-posterior communicating artery aneurysm. The neck of the aneurysm was clipped successfully and the post-operative period was uneventful. However, two months after discharge, the patient reported that her mental status had declined over previous weeks. A cranial computed tomography scan revealed an interval increase in the size of the ventricle and arachnoid cyst causing a midline shift. Simultaneous navigation guided ventriculoperitoneal shunt and cystoperitoneal shunt placement resulted in remarkable radiological and clinical improvements.
INTRODUCTION
Several reports on intracranial arachnoid cysts (ACs) have placed special emphasis on their association with hydrocephalus, and in the majority of these reports an effort was made to explain the linkage between hydrocephalus development and ACs.5)11)12) However, somewhat surprisingly, little is known about the association between a preexisting AC and acquired hydrocephalus in aneurismal subarachnoid hemorrhage (SAH). Furthermore, to the best of our knowledge, no case of communicating hydrocephalus accompanied by AC in aneurismal SAH has been reported. We report a unique case of communicating hydrocephalus accompanied by an AC in aneurismal SAH.
CASE REPORT
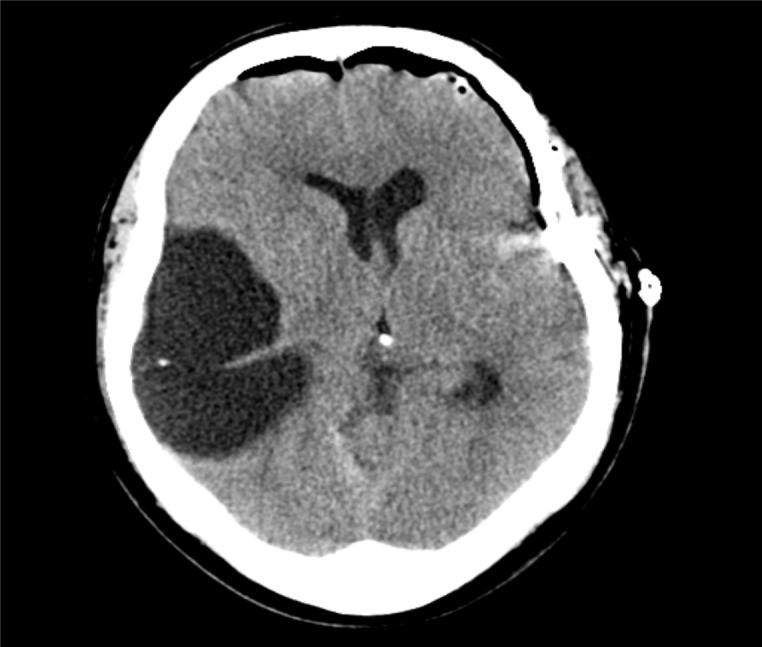
A 69-year-old female with no significant prior medical history was referred to our clinic due to a headache of sudden onset. Head computed tomography (CT) scan performed at the time demonstrated an AC in the right middle fossa with a mass effect and diffuse SAH (Fig. 1). On clinical examination, the patient appeared lethargic and drowsy with a Glasgow coma scale score of 13 (E3, M6, V4), a Hunt-Hess grade of III, and a Fisher grade of IV.

The initial computed tomography (CT) scan shows a large, hypodense lesion within the right middle cranial fossa, causing a midline shift with right lateral ventricle compression, and scanty subarachnoid hemorrhage in the left sylvian fissure.
Left carotid angiography revealed a left internal carotid-posterior communicating artery aneurysm, with a postero-laterally projecting dome (Fig. 2). Craniotomy was performed and complete aneurysm neck clipping and posterior communicating artery patency were confirmed intraoperatively by ultrasound using a micro-Doppler probe (Fig. 3). The post-operative period was uneventful. The patient's consciousness level gradually improved, and she was discharged on the 17th post-operative day. However, at two months after discharge, she reported that her mental status had been declining over recent weeks. A neurological examination performed at the time revealed decreased consciousness, that is, severe confusion with gait disturbance and urinary incontinence. Cranial CT revealed an interval increase in the size of the ventricle and an AC causing a midline shift (Fig. 4). We planned simultaneous ventriculoperitoneal shunt and cystoperitoneal shunt placement to correct the enlarged ventricle and AC. The patient was positioned supine with her head turned left to expose the right temporal scalp. A curvilinear skin incision was made over the temporo-occipital scalp for cyst access and another linear incision was made on the right Kocher's point for ventricular access by an intraoperative neuro-navigation system. Two intracranial catheters were connected using a Y-shaped titanium connector at the gate of the single valve (Fig. 5). A linear skin incision was made in the right upper abdomen to access the peritoneum for the distal end of the shunt catheter, and a programmable valve and distal catheter were tunnelled and passed in the usual manner.

Left internal carotid angiogram depicting a left internal carotid-posterior communicating artery aneurysm projecting posteriorly and laterally.
Postoperative CT scan showing decreased ventricle size.
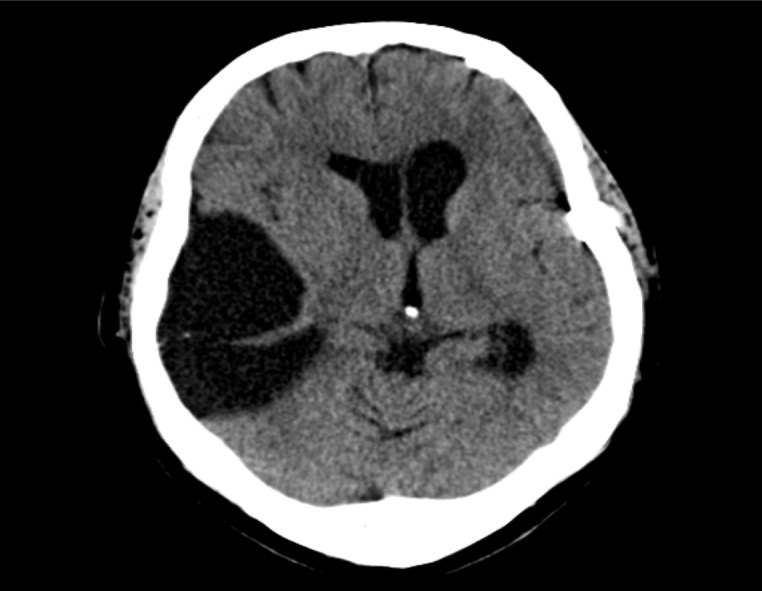
CT scan obtained two months after operation showing an interval increase in ventricle and arachnoid cyst sizes causing a midline shift.
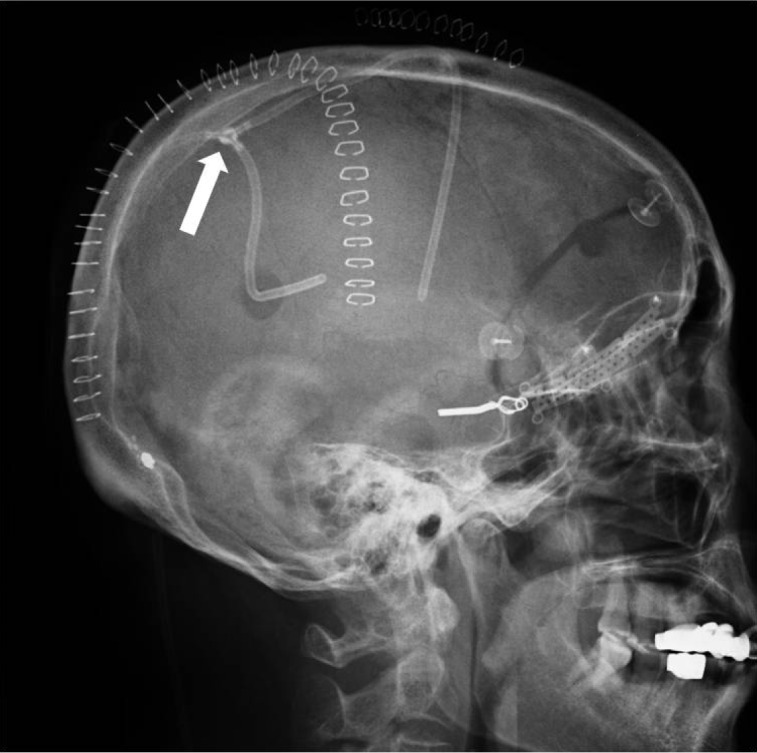
Lateral skull radiograph demonstrating 2 intracranial catheters in the cyst and lateral ventricle connected by a titanium Y-shaped connector (arrow) at the gate of the single valve.
The neurological deficits gradually subsided after the procedure and, two weeks later, the patient was discharged to home with no neurological deficit. Follow-up CT performed at one year post-operatively showed proper positioning of the shunt components and an interval improvement in brain condition including the hydrocephalus (Fig. 6).

Follow-up CT scans obtained at about one year post-operatively show proper positioning of shunt components (A) and an interval decrease in ventricles and cyst sizes (B).
DISCUSSION
Intracranial aneurysms and ACs are relatively common cerebral malformations, but coincidental occurrence between these two disorders are rare.3)14) Including our new case, only ten cases have been published.1)2)6-8)10)13)14) Hirose et al.6) were the first to reported a case of intracystic hematoma without SAH due to a ruptured aneurysm. Similarly, Kajiwara et al.9) described a case of AC in the middle fossa with intracystic hematoma caused by the rupture of an aneurysm arising from the internal carotid-posterior communicating artery. Furthermore, it was recommended that the coexistence of AC and a ruptured aneurysm be considered, indicating the need for cerebral angiography to investigate an intracystic hematoma of an AC, especially in the absence of head injury. However, although most authors have described the characteristics of hemorrhage due to aneurismal rupture in a case of coexistent AC, no mention has been made of the effect of a preexisting AC with hydrocephalus occurring after aneurismal SAH or their interactions.
Depending on the size of the cystic opening and on cerebrospinal fluid (CSF) dynamics, ACs may be classified as communicating or non-communicating according to their relationships with subarachnoid spaces. ACs may expand by the following mechanisms: (a) by a ball-valve action that allows the entry of CSF into a cyst but prevents egress, (b) by the intracystic production of fluid by secreting cells, occasionally found in the cyst walls, or (c) by movements of fluids driven by osmotic gradients.11)
In the present case, we believe that the middle fossa AC communicated with subarachnoid space and was asymptomatic before the aneurismal SAH, but that delayed hydrocephalus resulting from the aneurismal SAH inflated the middle fossa AC gradually and caused a midline shift. We recall that her mental status at the time of the shunt operation was worse than usually encountered in patients suffering from delayed hydrocephalus after aneurismal SAH. Therefore, we suggest that a preexisting communicating AC can exacerbate the symptoms of hydrocephalus after SAH because of the mass effect of the expanded AC.
With regards to treating hydrocephalus in this case, at first we considered a ventriculoperitoneal shunt or cystoperitoneal shunt independently because we believed that there was communication between the cyst and subarachnoid space. However, some authors suggest that preceding or coexistent hydrocephalus is important in AC expansion,4)12) explaining the development of ventriculomegaly or hydrocephalus following cyst shunting or, on the contrary, AC growth following the extracranial drainage of ventricular CSF.12) However, we were concerned about unpredictable changes in CSF dynamics after single shunt placement, and thus, finally decided on simultaneous ventriculoperitoneal shunt and cystoperitoneal shunt placement to treat the enlarged ventricle and AC. Fortunately, the result of surgery was highly satisfactory both clinically and radiologically.
CONCLUSION
We document an uncommon case of communicating hydrocephalus accompanied by AC in aneurismal SAH, describe its clinical features, and include a review of the literature. This case demonstrates that a preexisting communicating AC can exacerbate the symptom of hydrocephalus occurring after aneurismal SAH because of the mass effect of the expanded AC.
Notes
This work was supported by a clinical research grant from Pusan National University Hospital 2012.