



INTRODUCTION
Transvenous embolization is an effective treatment option for cavernous sinus dural arteriovenous fistulas (CDAVFs) [13]. Inferior petrosal sinus (IPS) is the most commonly used venous route for the treatment; other routes include the superior ophthalmic vein (SOV), superior petrosal sinus, pterygoid venous plexus, inferior petrooccipital vein, and intercavernous connections [4]. In cases with IPS occlusion, other venous approaches should be attempted to access CDAVF. A few reports have suggested using the trans-facial vein approach or direct percutaneous transorbital puncture of the SOV or inferior ophthalmic vein [6].
In the case presented below, we adopted a rare transvenous approach to the CDAVF via the middle temporal vein (MTV) as IPS was not accessible.
DESCRIPTION OF CASE
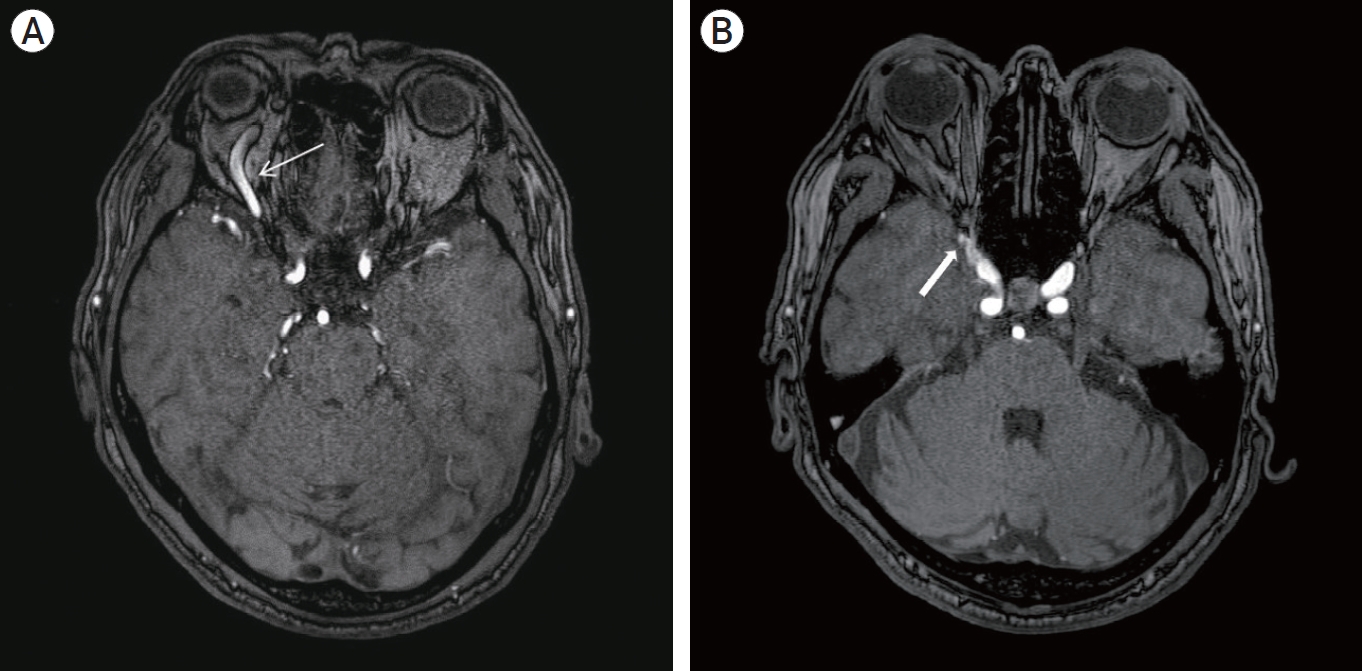
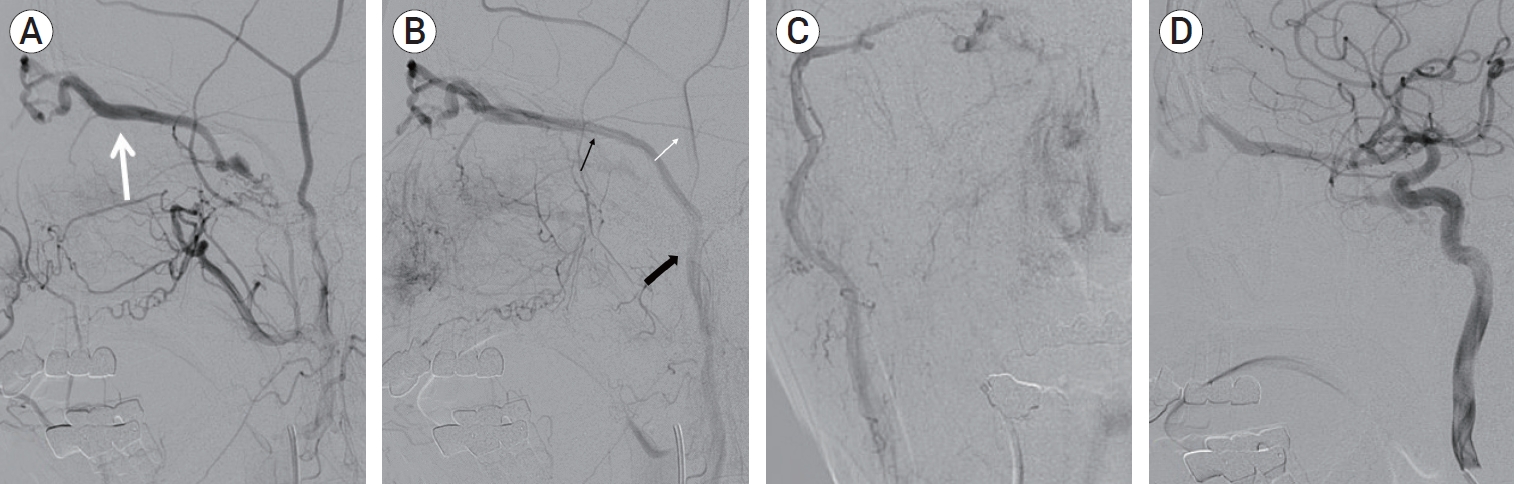
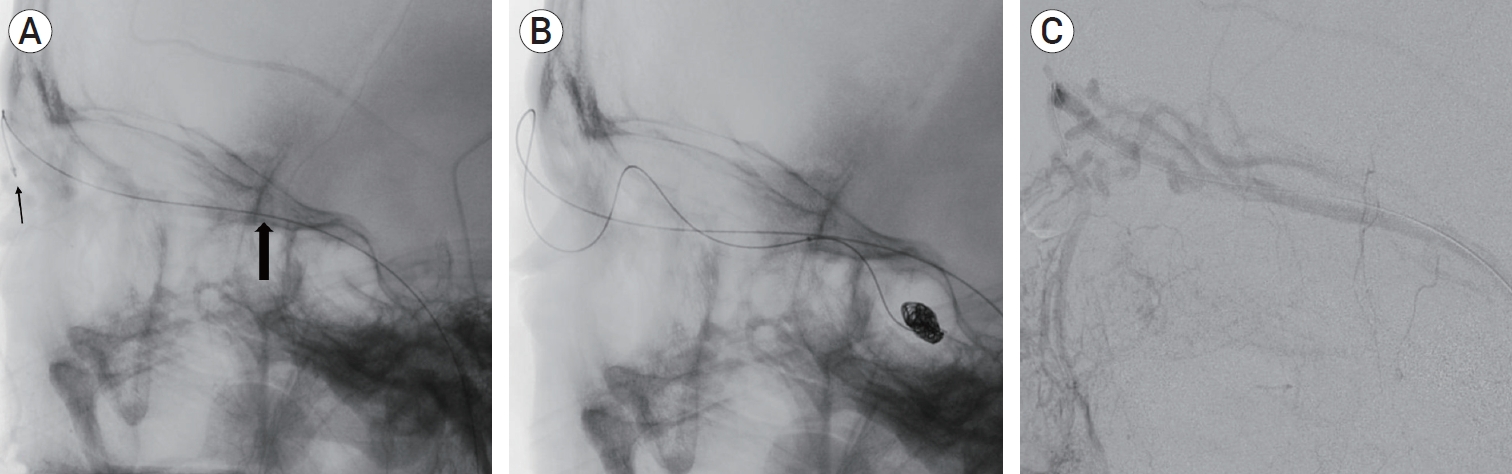
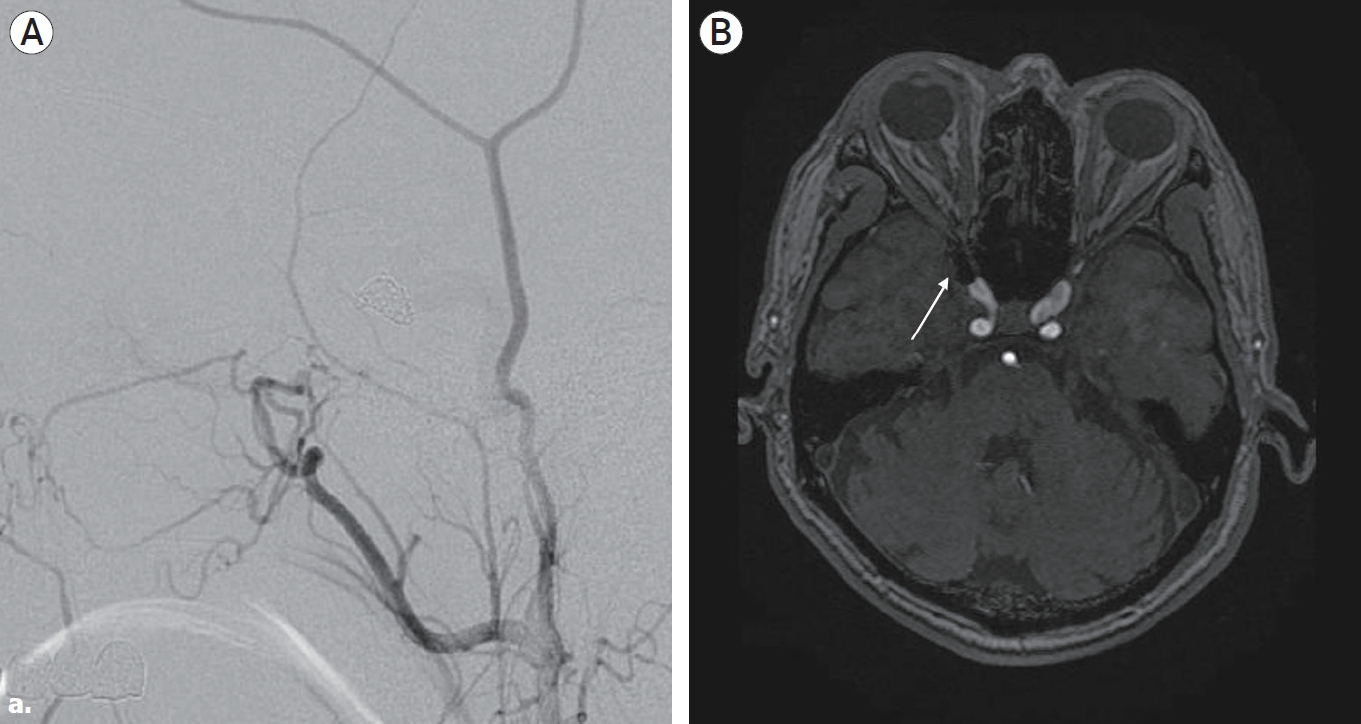
A 65-year-old man presented with unilateral blurred vision in the right eye, chemosis, exophthalmos, and bruit for one month. There was no history of trauma, infection, or skull-base surgery. He visited the ophthalmology outpatient department and was treated conservatively; however, it was not effective. Magnetic resonance angiography (MRA) revealed a dilated SOV with prominent vascularity in the right anterior cavernous sinus region, suggesting CDAVF (Fig. 1). Digital subtraction angiography (DSA) confirmed the presence of CDAVF with prompt opacification of the SOV with venous reflux. Multiple arterial feeders supplied the CDAVF, including foramen rotundum artery through internal maxillary artery, and distal dural branch of the inferolateral trunk through internal carotid artery. CDAVF had predominant venous drainage toward the SOV, which drained into the MTV (Fig. 2). IPS, presumably thrombosed, was not observed. Although the angiogram showed indirect CDAVF, the patient showed persistent blurred vision symptoms, and we decided to treat it through transvenous embolization. During the procedure, both the femoral artery and vein were punctured, a 5 F sheath was placed in the artery, and a 6 F sheath was placed in the femoral vein. And 6 F Envoy guiding catheter (Codman & Shurtleff, Rayham, MA, USA) was advanced to the external jugular vein just before the entrance of the retromandibular vein, thus microcatheter was accessed through the retromandibular vein. The headway 17 advanced microcatheter (MicroVention, Valencia Avenue Tustin, CA, USA) was placed at the distal MTV and advanced to the cavernous sinus via the nasofrontal vein and SOV (Fig. 3A). Then, it could finally enter the venous pouch of the arteriovenous fistula, which was completely obliterated with detachable coils packed within the venous pouch (Fig. 3B). After the endovascular treatment, DSA showed complete occlusion of the CDAVF (Fig. 4A). A detachable coil was observed on postoperative MRA near the right anterior cavernous sinus (Fig. 4B). The patientŌĆÖs symptoms improved, and the postoperative course was uneventful. Follow-up MRA obtained one year after treatment showed persistent occlusion of the arteriovenous fistula.
DISCUSSION
We searched for literature using the PubMed database (until May 2021) to identify studies in humans that described an MTV approach to treat CDAVF and examined the clinical outcomes. To maximize search sensitivity and identify all relevant studies, combinations of terms, such as ŌĆśMTV,ŌĆÖ ŌĆśsuperficial temporal vein,ŌĆÖ ŌĆśsuperior ophthalmic vein,ŌĆÖ ŌĆścarotid cavernous fistula,ŌĆÖ ŌĆśtrans-venous approach,ŌĆÖ and ŌĆśembolizationŌĆÖ were searched as either keywords or Medical Subject Headings (MeSH) terms. Furthermore, reference lists of all retrieved articles were reviewed to identify potentially relevant studies.
The articles identified were systematically assessed for inclusion in our review. Studies in which the patients had CDAVF and the treatment plan was transvenous embolization via a superficial middle temporal approach were included. Studies describing various transvenous approaches for CDAVF were included if the outcomes of the middle temporal approach group were reported separately. Reports describing transvenous approaches, including inter-cavernous, direct SOV, sphenoparietal sinus, superior petrosal sinus, and pterygoid plexus, were excluded. All the included publications were available in the English language.
A total of 75 articles were identified using the search criteria. After applying the eligibility criteria, eight studies were included in the final review (Table 1). Twenty patients underwent CDAVF treatment via a MTV approach. Overall, 23.6% of the patients were men, and the weighted average age of all patients was 58.1 years. The primary approach used for the MTV approach was transvenous embolization via the SOV, performed in 20 patients. The direct MTV approach was described in four cases, and all others used a transfemoral approach.
CDAVF is an abnormal communication between the cavernous sinus and the nearby arterial system [5]. It is the most commonly involved site in intracranial dural arteriovenous fistulas [11]. CDAVF has a wide variety of symptoms, depending on the route of venous drainage, pouch location, and size [20]. Venous reflux into the ophthalmic vein can lead to orbital venous hypertension, resulting in increased intraocular pressure and intraorbital fluid retention. These abnormalities eventually lead to visual (e.g., diminished visual acuity and visual loss) and ocular (e.g., exophthalmos, proptosis, chemosis, subconjunctival hemorrhage, and corneal damage) symptoms. Venous reflux into the IPS causes symptoms, such as tinnitus or bruit. Venous reflux into the middle cerebral vein can cause seizures or hemorrhage due to venous congestion and infarction. Cranial nerve deficits, such as ptosis, diplopia, anisocoria, and ophthalmoplegia, may occur due to the steal phenomenon of the nerveŌĆÖs vascular supply [16].
In CDAVF, invasive treatment can be considered when visual symptom degeneration or intolerable pain occurs [9]. Various treatment modalities, including direct surgery, radiosurgery, and endovascular access (transarterial or transvenous embolization), have been proposed to treat this pathology [15]. In patients with mild symptoms, conservative management and external manual carotid compression can be considered. Among these methods, transvenous embolization is now accepted as the first treatment for most symptomatic CDAVFs.
IPS, one of the most commonly used transvenous pathways for embolization, has the advantage of easy access to the cavernous sinus due to its short and straight course. However, if the cavernous sinus is not accessible through the IPS due to occlusion, thrombosis, anomaly, or cavernous sinus compartmentalization, other pathways must be considered for CDAVF embolization. Several alternative venous routes are available: through the medial side of the lesion, the anterior or posterior intercavernous sinus can be attempted via the contralateral cavernous sinus; the passageway to the anterior side of the lesion through the SOV; the anterosuperior side, which can be accessed through the sphenoparietal sinus; the posterior side can be accessed through the superior petrosal sinus; and finally, the inferior side can be accessed through the pterygoid plexus.
The SOV, a frequently considered pathway when the IPS is occluded, can be accessed through the facial vein and has a high success rate [1]. If the facial veins are not sufficiently dilated in the endovascular approach, a direct surgical approach to the SOV or inferior ophthalmic vein is possible [21]. However, it can be tedious, difficult, and has potential complications, such as acute exophthalmos and subsequent visual loss [3,8]. Therefore, even though it is a tortuous pathway, the approach through the surrounding venous channel (trans-femoral or peripheral approach) is preferred because it has the advantage of being safe and having fewer side effects.
When an IPS approach is not available for the transvenous embolization treatment of a CDAVF, the use of the SOV via the MTV as an alternative route has rarely been reported (Table 1). It may be difficult to get through venous catheterization of the SOV via the MTV because of its narrow caliber, tortuous course, and formation of an acute angle at the junction of the MTV, nasofrontal vein, and SOV. However, a venous approach through this location was not impossible [7]. We also had difficulties placing the catheter in the procedure, but could insert the guiding catheter by bending it into a J-shape and pushing it in gently. DSA often showed MTV dilatation and straightening; therefore, these venous channels provide an alternative route for transvenous embolization. Dilated MTV has been previously reported in other studies that treated CDAVF using the MTV approach [18]. In CDAVF with characteristic retrograde venous drainage and ocular symptoms, MTV dilatation is frequently observed due to venous reflux and hypertension through the SOV [20]. Therefore, the venous channel provide an alternative route for transvenous embolization, and it is necessary to identify superficial middle temporal venous approach routes when planning endovascular treatment.
The veins that are located on the lateral aspect of the skull include the superficial temporal vein (STV), MTV, and transverse facial vein (TFV), which share the same running path as the artery with a similar name. MTV is the frontal branch of the STV and connect to the SOV through the nasofrontal vein and can access the cavernous sinus (Fig. 2B). It can be confused with the TFV, but TFV travels to the inferior border of zygoma, similar to transverse facial artery. The STV drains into the retromandibular vein and eventually flows into the common facial vein. The average MTV diameter was 1.88-3.1 mm. MTV branched out from the superficial temporal vein at 12.7┬▒6.6 mm above the upper border of the zygomatic arch and ran 52.0┬▒6.5 mm to the bony lateral canthus [17]. In our case, the diameter of the MTV showed an extended finding of 3.5 mm.
A total of 20 CDAVF patients, summarized in Table 1, and our patient was also treated using the MTV approach. Access through the femoral vein was performed in 16 cases, and direct MTV puncture was performed in 4 cases. In the approach pathway, depending on the anatomical variation, the external or internal jugular vein can access the MTV. Neither our patient nor the reviewed cases (Table 1) reported any perioperative or postoperative complications. It is evident that this is a safer method than the direct ophthalmic puncture procedure. Compared with other alternative approach methods, no studies describing the complete occlusion rate were found; however, in review of the other cases of using the MTV approach, all of the cases except for the 7 cases that did not describe the results showed complete occlusion. Complete occlusion seemed sufficiently possible in treatment of CDAVF via MTV approach [18].
Therefore, when IPS occlusion and venous reflux to SOV are present in CDAVF patients, MTV dilatation can often be observed, and an approach using MTV can be provided as a sufficiently safe and effective method to treat CDAVF.
CONCLUSIONS
Transfemoral catheterization of the cavernous sinus via the MTV is a safe and effective approach, which increases technical success by providing an alternative route for transvenous embolization of CDAVF when other venous routes, such as IPS, are difficult or impossible to navigate with a catheter. Therefore, we should be aware of the presence of MTV on a diagnostic angiogram when it is challenging to reach CDAVF through the conventional route.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






