



INTRODUCTION
Dizziness triggered by rotating the head is a characteristic symptom of rotational vertebral artery syndrome (RVAS). However, dizziness has many causes, and patients who complain of dizziness provoked by rotating the head should also be evaluated in terms of a peripheral disorder, such as benign paroxysmal positional vertigo (BPPV). Videonystagmography (VNG) is useful for distinguishing between peripheral disorder and central disorder (1,2). There are various treatment options, ranging from conservative treatment such as rehabilitation to surgery (3). Decompression without fusion is the recommended first-line therapy and a posterior approach is generally preferred to decompress the VA at the C1-2 level (4,5,6). We present a case of RVAS diagnosed via VNG, CTA and three-position DSA. The exact stenotic point was determine based on three-position DSA. The patient was treated via anterior VA decompression at the C2 transverse foramen, not posterior approach. A satisfactory outcome was achieved.
CASE DESCRIPTION
A 38-year-old male suffering from alcoholism visited our outpatient department complaining of repeated dizziness and a buzzing sound in the left ear. His first ear symptom was a hearing difficulty commencing 1 year prior. Dizziness and a buzzing sound developed when he turned his head to the right, commencing a few months prior. Sometimes, the dizziness was so severe that he could not open his eyes. Then, he failed to maintain balance and fell, losing consciousness for 3-4 seconds. On examination, we found that the symptoms appeared only when he turned the head to the right, whether he was standing, sitting, or lying. No symptoms were evident when the head was rotated to the left or in the neutral position. A down-beat nystagmus appeared when the head turned to the right.
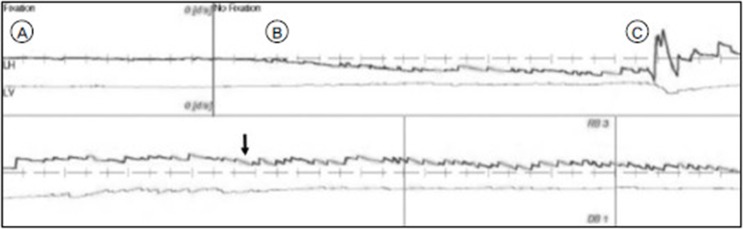
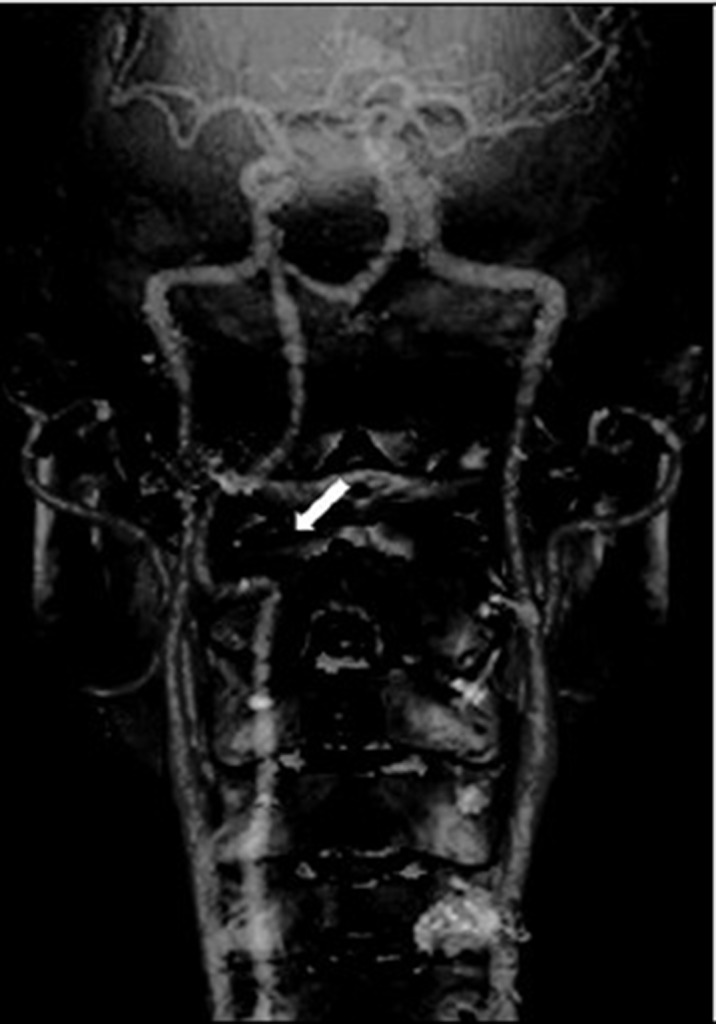
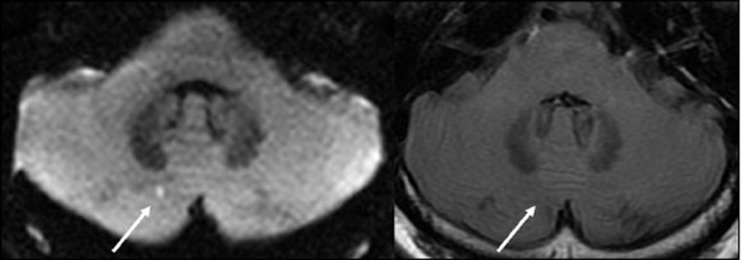
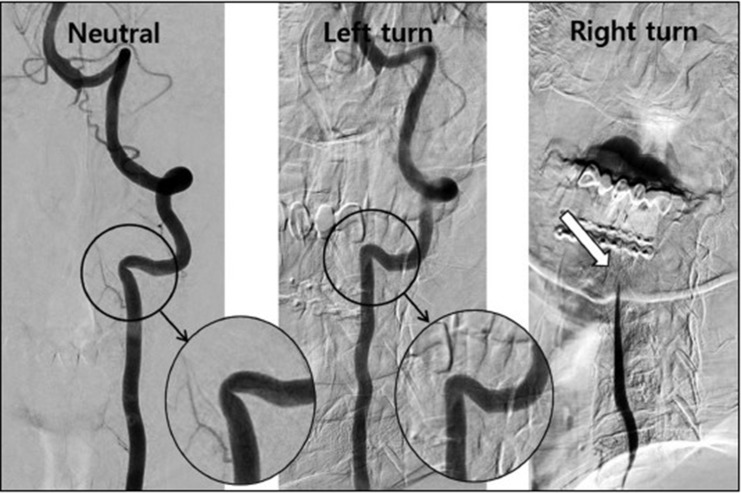
We used VNG to determine whether the problem was peripheral or central. VNG revealed right-beating nystagmus with a down-beat component when the head was turned to the right (Fig. 1), indicating a central rather than a peripheral origin. We scheduled brain and neck CTA, brain MRI, and three-position DSA to evaluate central origin. CTA revealed a hypoplastic right VA and left VA stenosis at the lateral curvature of the VA at C2 transverse foramen. (Fig. 2) Brain MRI revealed a tiny, acute ischemic infarction in the right cerebellum. (Fig. 3) DSA was performed in three positions (with the head neutral, 90° to the left, and 90° to the right). In the neutral position, left VA stenosis was observed at the C2 transverse foramen, as on CTA. Notably, when the head was turned to the left, the VA stenotic lesion became wider than in the neutral position. When the head was turned to the right, the blood flow tapered at the C3-4 level and was totally occluded at the C2 level. (Fig. 4) Few minutes after angiography with 90° to the right, the patient lost consciousness and DSA was halt. As the right VA was hypoplastic and flow almost absent, the posterior circulation was highly dependent on the left VA. We concluded that the left VA became kinked at the C2 transverse foramen when the head was turned to the right. We decided to perform anterior decompression of the left VA.
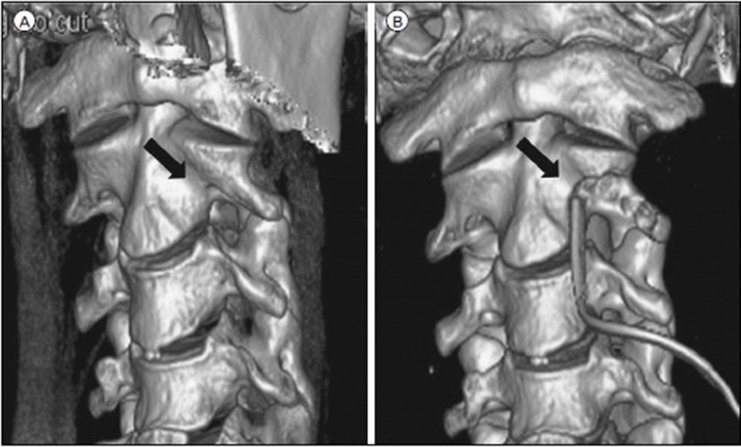
The patient was placed in the supine position and a transverse skin incision was created on the medial border of the sternocleidomastoid muscle at the C2-3 level. The anterolateral portion of the left transverse foramen that covered the VA was carefully drilled. The VA was fully decompressed, and VA pulsation immediately became more active. Postoperative CTA showed a wider transverse foramen than preoperatively (Fig. 5). The symptoms improved dramatically after surgery. Neck movement was not limited, and no instability was noticed on a dynamic X-ray of cervical spine.
DISCUSSION
It is challenging to distinguish between nystagmus of peripheral and central origin; this requires consideration of various clinical symptoms and features. The direction of nystagmus after a positioning maneuver can point to a central disorder. Paroxysmal down-beat, up-beat, or pure torsional nystagmus is considered to reflect a central origin (2,7). Our patient's nystagmus contained a down-beat component, and thus was not exclusively right-beating, suggesting a central origin. We were able to determine the need for CTA and DSA at risk of radiation exposure and invasive using VNG, a non-invasive and radiation free test.
Rotatory VA stenosis at the C1-C2 level with reduced blood flow can be observed in normal individuals, reflecting relative immobilization of the VA at the C2 and C1 transverse foramina. During head rotation, the atlantoaxial joint is fixed, whereas the C1 contralateral transverse foramen moves forward and downward, kinking the contralateral VA at the transverse foramen and stretching the extraspinal VA segment, decreasing blood flow (8,9). This does not normally trigger infarction of the posterior circulation because the remaining contralateral VA and the anastomosis confer adequate circulation (10). If the opposite VA is hypoplastic or rendered stenotic or occlusive by arteriosclerotic changes, the posterior circulation is vulnerable to infarction in most RVAS cases (3). In the case reported here, as the right VA was hypoplastic and flow almost absent, the posterior circulation was highly dependent on the left VA. We concluded that when the head was turned right the left VA became kinked at the C2 transverse foramen.
The anatomical course of the VA was the most important factor when choosing an approach (4,5). The VA moves anteriorly from C6 to C3 after passing the lateral curvature at C2, and then ascends sharply posteriorly. The VA at C1-2 is best visualized via a posterior approach and below C3 via an anterior approach. Although a posterior approach is generally preferred to decompress the VA at the C1-2 level, some reports described successful decompression via an anterior approach (11,12). In our case, the stenotic lesion lay at the C2 transverse foramen not in the C1-2 joints therefore it is best visualized via anterior approach. It is important to choose the surgical approach that best visualized exact stenotic point, rather than simply determined by the stenotic level.
CONCLUSION
A patient with repeated dizziness and syncope was diagnosed with RVAS. Down beating nystagmus on VNG indicated origin of dizziness was central. The three-position DSA showed the stenotic point of VA became narrowed and widened according to the head rotation. The precise stenotic point evaluation by three-position DSA is crucial for the planning of surgical treatment.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






